14/09/2014
HEA: Peut être un peu de sérénité ?
Hydroxyethyl Starches: A Tale of Two Contexts: The Problem of Knowledge
Weiskopf R. Anesth Analg. 2014 Sep;119(3):509-13.
Un débat moins passionné est en train de se mettre en place au sujet de la toxicité des HES. Le texte proposé en est un exemple. Il propose une relecture pertinente des études 6S, CHEST et surtout CRISTAL qui d'une certaine façon remet en question les deux précédentes. Il nous demande de prendre en compte plusieurs éléments : La diversité des HES, les différences qui peuvent exister entre une administration répétée en réanimation et une administration ponctuelle péri-opératoire. Il s'appuie sur deux écrits publiés dans le même numéro.
Raghunathan K et all. (Intravenous Starches: Is Suspension the Best Solution?) suggèrent que les solutions colloïdes sont à réserver pour les hypovolémies aiguës alors que Irwin et all. (Volume Therapy with Hydroxyethyl Starches: Are We Throwing the Anesthesia Baby Out with the Intensive Care Unit Bathwater?) estiment que le recours aux HES 130/0.4 est pleinement justifié en environnement périopératoire.
Cette démarche correspond au positionnement de la SFAR. Rappelons que la position actuelle des instances européennes est la suivante:
" Les solutions à base d’HEA peuvent être utilisées pour la réanimation des patients avec une hypovolémie causée par une perte aiguë de sang, quand les alternatives comme la perfusion de cristalloïdes seuls sont insuffisantes. Afin de limiter les risques potentiels, les solutions contenant des HEA ne devront pas être utilisées plus de 24 heures et la fonction rénale devra être monitorée après administration des HEA "
| Tags : remplissage
14/12/2013
Kétamine: Son intérêt en médecine de guerre
Clic sur le document pour accéder au document.
| Tags : kétamine
21/11/2013
Le plasma lyophilisé: Bon pour le cerveau du traumatisé qui saigne
Early treatment with lyophilized plasma protects the brain in a large animal model of combined traumatic brain injury and hemorrhagic shock
Imam AM et Al. J Trauma Acute Care Surg. 2013;75: 976-983
accéder aux abstracts de la WTA publiés dans J trauma Acute care
_____________________________________
Bien sûr une étude animale, mais une de plus qui milite pour un emploi précoce du plasma lyophylisé.
_____________________________________
BACKGROUND: Combination of traumatic brain injury (TBI) and hemorrhagic shock (HS) can result in significant morbidity and mortality. We have previously shown that early administration of fresh frozen plasma (FFP) in a large animal model of TBI and HS reduces the size of the brain lesion as well as the associated edema. However, FFP is a perishable product that is not well suited for use in the austere prehospital settings. In this study, we tested whether a shelf-stable, low-volume, lyophilized plasma (LSP) product was as effective as FFP.
METHODS:
Yorkshire swine (42-50 kg) were instrumented to measure hemodynamic parameters, intracranial pressure, and brain tissue oxygenation. A prototype, computerized, cortical impact device was used to create TBI through a 20-mm craniotomy: 15-mm cylindrical tipimpactor at 4 m/s velocity, 100-millisecond dwell time, and 12-mm penetration depth. Volume-controlled hemorrhage was induced(40-45% total blood volume) concurrent with the TBI. After 2 hours of shock, animals were treated with (1) normal saline (NS, n = 5), (2) FFP (n = 5), and (3) LSP (n = 5). The volume of FFP and LSP matched the shed blood volume, whereas NS was 3 times the volume. Six hours after resuscitation, brains were sectioned and stained with TTC (2, 3, 5-Triphenyltetrazolium chloride), and lesion size (mm3) and swelling (percent change in volume compared with the contralateral, uninjured side) were measured.
RESULTS:
This protocol resulted in a highly reproducible brain injury, with clinically relevant changes in blood pressure, cardiac output, tissue hypoperfusion, intracranial pressure, and brain tissue oxygenation. Compared with NS, treatment with LSP significantly ( p G 0.05) decreased brain lesion size and swelling (51% and 54%, respectively).
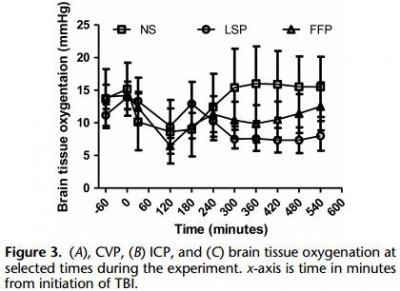
CONCLUSION: In a clinically realistic combined TBI + HS model, early administration of plasma products decreases brain lesion size and edema. LSP is as effective as FFP, while offering many logistic advantages.
| Tags : tbi, coagulopathie
16/11/2013
NAC après une explosion: Bon pour le neurone.
Amelioration of Acute Sequelae of Blast Induced Mild Traumatic Brain Injury by N-Acetyl Cysteine: A Double- Blind, Placebo Controlled Study
Hoffer ME et Al. PLoS One. 2013;8(1):e54163. doi: 10.1371/journal.pone.0054163. Epub 2013 Jan 23.
Background: Mild traumatic brain injury (mTBI) secondary to blast exposure is the most common battlefield injury in Southwest Asia. There has been little prospective work in the combat setting to test the efficacy of new countermeasures. The goal of this study was to compare the efficacy of N-acetyl cysteine (NAC) versus placebo on the symptoms associated with blast exposure mTBI in a combat setting.
Methods: This study was a randomized double blind, placebo-controlled study that was conducted on active duty service members at a forward deployed field hospital in Iraq. All symptomatic U.S. service members who were exposed to significant ordnance blast and who met the criteria for mTBI were offered participation in the study and 81 individuals agreed to participate. Individuals underwent a baseline evaluation and then were randomly assigned to receive either N- acetyl cysteine (NAC) or placebo for seven days.
4 g per os puis 18-24h après 2X2 g jusqu'à J4 puis 1,5 g X2 jusqu'à J7
Each subject was re-evaluated at 3 and 7 days. Outcome measures were the presence of the following sequelae of mTBI: dizziness, hearing loss, headache, memory loss, sleep disturbances, and neurocognitive dysfunction. The resolution of these symptoms seven days after the blast exposure was the main outcome measure in this study. Logistic regression on the outcome of ‘no day 7 symptoms’ indicated that NAC treatment was significantly better than placebo (OR = 3.6, p = 0.006). Secondary analysis revealed subjects receiving NAC within 24 hours of blast had an 86% chance of symptom resolution with no reported side effects versus 42% for those seen early who received placebo.
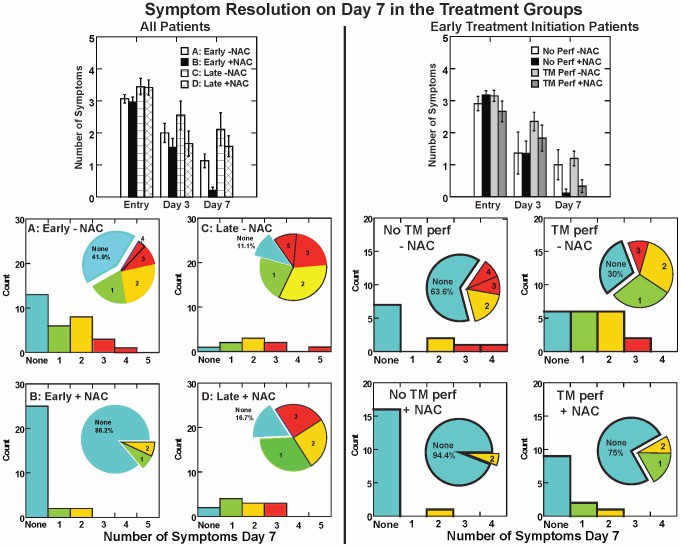
Conclusion: This study, conducted in an active theatre of war, demonstrates that NAC, a safe pharmaceutical countermeasure, has beneficial effects on the severity and resolution of sequelae of blast induced mTBI. This is the first demonstration of an effective short term countermeasure for mTBI. Further work on long term outcomes and the potential use of NAC in civilian mTBI is warranted
| Tags : blast
07/08/2013
Plasma: En préhospitalier AUSSI +++
Point-of-injury use of reconstituted freeze dried plasma as a resuscitative fluid: A special report for prehospital trauma care
Glassberg E. et All. J J Trauma Acute Care Surg. 2013;75(Suppl 2):S111YS111.
La prise en charge d'hémorrragie catastrophique en phase préhospitalière est particulièrement complexe. Ces dernières années la mise en place d'un réseau structuré de prise en charge, 'application de procédures spécifiques visant à arrêter les hémorragies au plus tôt, le recours à l'acide tranexaminique, la prévention des hypothermies et l'application d'une politique raisonnée de rénaimation/chirurgie ont constitué une grande avancée. Certaines nations ont équipé leurs vecteurs d'évacuations de concentrés érythrocytaires. Le maintien d'une coagulation optimale est un enjeu majeur. Pour cela existe, entre autres, le plasma lyophilisé. Les forces armées israéliennes militent pour l'emploi de ce type de solutions en phase préhospitalière
| Tags : coagulopathie, hémorragie
26/05/2013
Plasma lyophilisé: Une réalité
Le Service de Santé des Armées a recours depuis de nombreuses années (1, 2) à une présentation originale de plasma thérapeutique le PLYO.
Initialement réservé à un emploi en opérations extérieures, il vient d'être validé sous contraintes pour un usage sur le territoire national: Le plasma lyophilisé (PLYO) est principalement distribué aux unités médico-chirurgicales militaires déployées en Opérations Extérieures (OPEX) pour répondre aux contraintes logistiques du contexte opérationnel et à la nécessité de disposer, sans délai, de plasma pour le traitement des blessés hémorragiques. En milieu civil, le PLYO pourrait être utilisé par les établissements de santé présentant des difficultés logistiques majeures ne permettant pas d’assurer une chaîne du froid négative ou au cours de situations d’extrême urgence avec nécessité d’un apport de plasma thérapeutique sans délai. Dans cette deuxième indication, le PLYO devrait être utilisé en attendant que le plasma frais congelé soit décongelé et disponible. Le plasma lyophilisé français (PLyo®) préparé préférentiellement à partir de plasma frais congelé traité par l’amotosalen. Il est obtenu par lyophilisation à partir d’un mélange de PFC-IA issus d’aphérèse, provenant de dix donneurs différents au maximum, de groupes sanguins A, B, et AB, exempts d’anticorps immuns anti-A ou anti-B, conservés à une température inférieure ou égale à −25 °C.
Il en existe d'autres. Le plasma lyophilisé sud-africain (Bioplasma®) est le seul équivalent au monde du plasma lyophilisé français du fait de son universalité. Il s’agit d’un produit sud-africain bénéficiant d’une autorisation nationale depuis 1994 et commercialisé depuis 1996. Ce plasma est lyophilisé, universel et traité par solvant-détergent. Il existe en deux formats de flacon : 50 ou 200 mL. Le plasma lyophilisé allemand (LyoPlas N-W®), produit par le service de transfusion sanguine de la croix rouge allemande, provient d’un seul donneur de sang total ou d’aphérèse. Il n’est donc pas universel au regard de la compatibilité ABO. Le produit est sécurisé par quarantaine de quatre mois. Il peut être stocké 15 mois entre +2 et +25 °C.
Une révue récente fait le point sur les divers plasma thérapeutiques disponibles.

| Tags : coagulopathie
21/02/2013
Pour la coagulation: HEA de haut PM pas bon ?
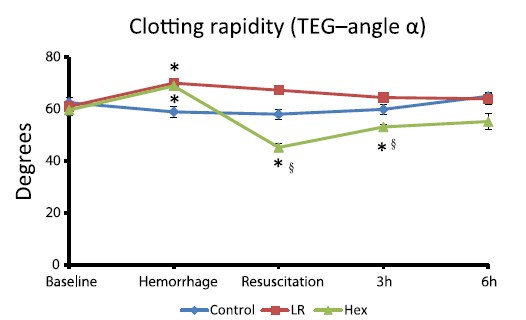
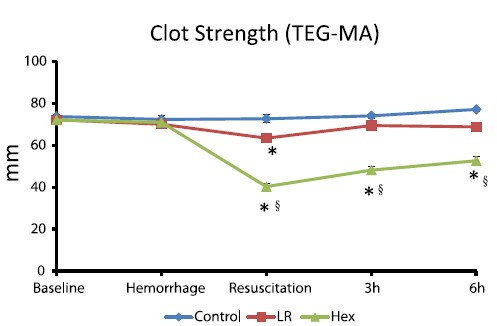
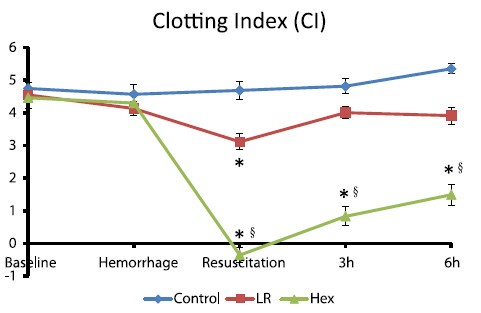
Comparisons of lactated Ringer’s and Hextend resuscitation on hemodynamics and coagulation following femur injury and severe hemorrhage in pigs
Wenjun Z et all J Trauma Acute Care Surg. 2013;74: 732-740
After traumatic hemorrhage, coagulation function was restored within 6 hours with LR resuscitation but not with Hextend. The lack of recovery after Hextend is likely caused by greater hemodilution and possible effects of starches on coagulation substrates and further documents the need to restrict the use of high-molecular-weight starch in resuscitation fluids for bleeding casualties.
On rappelle que l'Hextend est un HEA 670/0.75 et que le voluven est un HEA 130/0,4 dont les effets sur la coagulation sont réputées étant moindres.
| Tags : coagulopathie, remplissage, hémorragie
02/01/2013
Kétamine: La bonne dose pour le bon usage
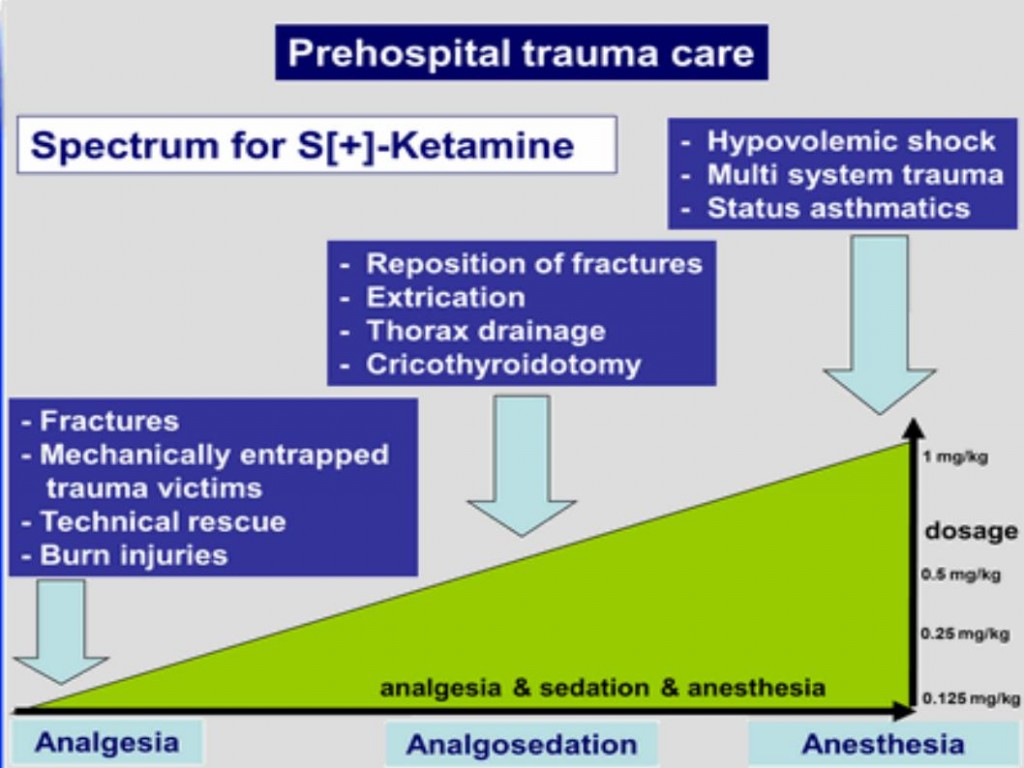
Josse F SOMA 2011
02/12/2012
Hémostase et transfusion par A. Godier IAR IDF

CLIC sur le logo pour accéder au cours
| Tags : hémorragie
01/12/2012
Apport du fibrinogène: A la folie ou pas du tout ??
Une econférence qui fait parfaitement le point sur l'intérêt et les questions en suspens concernant l'intérêt du fibrinogène dans la réanimation hémostatique du traumasié qui saigne.
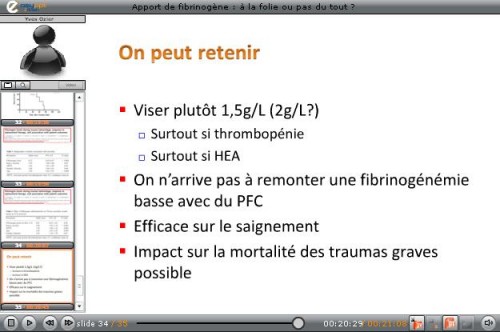
En condition de combat avant l'arivée en structure hopsitalière de campagne, l'apport de fibrinogène peut être réalisé par l'apport de plasma lyophylisé (PLYO) produit par le SSA (obtenu en moins de 6 min après reconstitution à température ambiante par adjonction d'eau PPI, chaque unité contient au moins 0,5g de fibrinogène). C'est une des composantes de la transfusion de plasma thérapeutique. qui doit désormais être envisagé au niveau du role 1 (poste de secours ou vecteur d'évacuation tactique).
Le recours au fibrinogène (Clottafact), qui apparaît être d'un intérêt majeur compte tenu d'un apport insuffisant par la transfusion de plasma. (Abstract Rourke et all.)
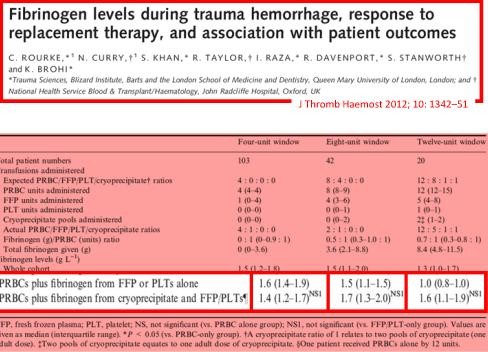
Il ne peut (pour des raisons de logistique de production et de disponibilté) être apporté qu'à partir de la prise en charge hospitalière.
Pour approfondir avec en perspective le blessé de guerre hémorragique:
(1) Un revue générale sur la coagulopathie de l'hémorragie massive: "Hemodilution caused by trauma and major surgery induces complex hemostatic changes involving procoagulant factors as well as anticoagulant, fibrinolytic, and antifibrinolytic factors. The endothelial responses to shear stress, active proteases, and various inflammatory cells and cytokines add further complexity to the pathophysiology of massive hemodilution. In addition to the conventional transfusion products, which are often difficult to administer in a timely manner, purified factor concentrates of plasma origin and from recombinant synthesis are highly concentrated (i.e., small volume) for a rapid restoration of targeted factor(s). The use of point-of-care testing is desirable to optimize the dose and timing of such intervention. Additional clinical trials of different factor concentrate therapies are required to validate their efficacy and safety in patients after trauma or major surgery.152 Further understanding of the time course of pathophysiological changes in massive hemodilution is necessary to optimally balance hemostatic and anticoagulant therapies."
(2) Un focus sur le blessé de guerre: "In patients with combatrelated trauma requiring massive transfusion, the transfusion of an increased fibrinogen: RBC ratio was independently associated with improved survival to hospital discharge, primarily by decreasing death from hemorrhage. Prospective studies are needed to evaluate the best source of fibrinogen and the optimal empiric ratio of fibrinogen to RBCs in patients requiring massive transfusion."
(3) La stratégie transfusionnelle du blessé de guerre SFAR 2012: " En traumatologie, l’administration de fibrinogène est recommandée : dose initiale de 3 à 4 g suivie d’une administration régulière en cas d’hypofibrinogènémie biologique (<1,5 à 2 g/l) ou de signes thromboelastométriques de déficit fonctionnel en fibrinogène [8]. Une analyse nord-américaine rétrospective de 252 dossiers de BdG ayant nécessité une TM a permis de mettre en évidence qu’un apport faible de fibrinogène (< 0,2 g/CGR) au cours de la transfusion était associé à une majoration significative de la mortalité de ces blessés [39]. Le SSA américain utilise l’apport de cryoprécipités contenant surtout du fibrinogène et d’autres facteurs de coagulation pour compenser ces déficits [37]. Les recommandations du SSA français sont l’administration de fibrinogène de façon répétée afin de maintenir un fibrinogène plasmatique supérieur à 1,5 g/l ou en l’absence de laboratoire (situation des structures chirurgicales « légères »), d’administrer au moins 0,2 g de fibrinogène par CGR transfusé."
| Tags : coagulopathie
20/10/2012
Etomidate: Encore une méta-analyse à charge
Etomidate is associated with mortality and adrenal insufficiency in sepsis: A meta-analysis.
Chee Man C. et all. Crit Care Med 2012;40:2945–2953
L'étude kETASED a confirmé l'intérêt du recours à la Kétamine chez le patient en défaillance vitale. Il existe une polémique concernant les effets délétères de l'étomidate sur la fonction corticosurrénalienne. Bien qu'une analyse récente n'ait pu l'objectiver après administration unique, la controverse continue. Une méta-analyse incluant chez 865 patients porteur de sepsis plaide pour l'existence d'une telle surmortalité.
On rappelle qu'en condition de combat, au delà de ce débat, l'agent d'induction de choix est la kétamine car son intérêt ne se limite pas à la simple induction. C'est aussi un agent de sédation et un antalgique.

23/09/2012
Facteur VIIa: Intérêt pas prouvé !
Use of recombinant factor VIIA for control of combat-related haemorrhage.
Woodruff SI et all. Emerg Med J 2010;27:2 121-124
Ce travail met en exergue que le recours au FVIIa n'a pas d'intérêt prouvé en cas de prise en charge de traumatismes pénétrants. Ceci est d'autant plus vrai qu'il est fait alors qu'une coagulopathie sévère est installée (The utility of recombinant factor VIIa as a last resort in trauma. Mamtani R. et all. World Journal of Emergency Surgery 2012, 7(Suppl 1):S7)
----------------------------------------------
Background
Recombinant activated human coagulation factor VII (rFVIIa), an intravascular strategy to promote clotting, is being used as an adjunct to surgical control of bleeding in combat trauma patients.
Objective
To describe the initial experiences with rFVIIa administered to combat casualties at US Navy-Marine Corps medical treatment facilities in Iraq, and to comparesurvival outcomes of those treated with rFVIIa to controls not receiving rFVIIa.
Methods
Medical encounter data from the US Navy-Marine Corps Combat Trauma Registry were retrospectively reviewed to identify all battle-injured patients documented as having received rFVIIa during the period May 2004 to January 2006 of Operation Iraqi Freedom. Available clinical and injury related data are presented to characterise the patients. To assess effects of rFVIIa on survival outcomes, rFVIIa cases were matched to controls on injury severity and age.
Results
22 battle-injured patients from the Combat Trauma Registry received rFVIIa. Primarily young US Marines, these patients typically had penetrating injuries from improvised explosive devices and gunshot wounds. Injuries were often abdominal. The average dose used was similar to that reported in another study of civilian trauma patients, although dosing varies widely in the existing experimental and anecdotal literature. Over two-thirds (68%) of the rFVIIa patients surviveddan identical outcome seen for a matched control group of 22 patients.
Conclusions
Survival of seriously injured combat casualties was good, although identical to that of a control group. Methodological limitations of this retrospective study preclude making firm conclusions about the effectiveness of rFVIIa. Future controlled studies are needed for safety and efficacy testing of rFVIIa in combat trauma patients.
----------------------------------------------
| Tags : hémorragie, coagulopathie
27/05/2012
Extracteur d'O2 SAROS: Révolution ou Evolution ?
http://www.sequal.com/assets/File/9705COMPLETE_B%20web(1)...
Ce type d'extracteur est particulièrement intéressant par sa faible consommation énergétique rendant possible la production de 3 l/min d'un mélange à 93% d'oxygène en autonomie sur batterie à lithium. Cet extracteur est certifié aéronautique US

| Tags : oxygène
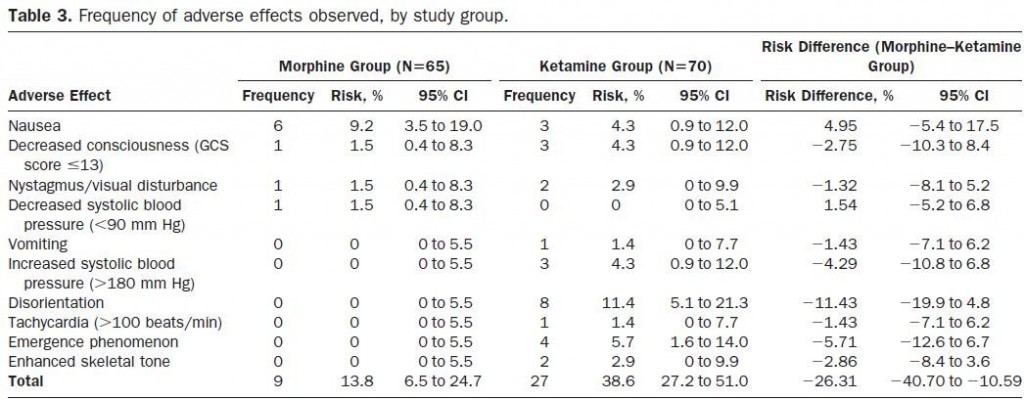
Morphine: Mieux avec UN PEU de kétamine
Morphine and Ketamine Is Superior to Morphine Alone for Out-of-Hospital Trauma Analgesia: A Randomized Controlled Trial
Jennings et all. Ann Emerg Med. 2012;59:497-503.
Study objective
We assess the efficacy of intravenous ketamine compared with intravenous morphine in reducing pain in adults with significant out-of-hospital traumatic pain.
Methods
This study was an out-of-hospital, prospective, randomized, controlled, open-label study. Patients with trauma and a verbal pain score of greater than 5 after 5 mg intravenous morphine were eligible for enrollment. Patients allocated to the ketamine group received a bolus of 10 or 20 mg, followed by 10 mg every 3 minutes thereafter. Patients allocated to the morphine alone group received 5 mg intravenously every 5 minutes until pain free. Pain scores were measured at baseline and at hospital arrival.
Results
A total of 135 patients were enrolled between December 2007 and July 2010. There were no differences between the groups at baseline. After the initial 5-mg dose of intravenous morphine, patients allocated to ketamine received a mean of 40.6 mg (SD 25 mg) of ketamine. Patients allocated to morphine alone received a mean of 14.4 mg (SD 9.4 mg) of morphine. The mean pain score change was −5.6 (95% confidence interval [CI] −6.2 to −5.0) in the ketamine group compared with −3.2 (95% CI −3.7 to −2.7) in the morphine group. The difference in mean pain score change was −2.4 (95% CI −3.2 to −1.6) points. The intravenous morphine group had 9 of 65 (14%; 95% CI 6% to 25%) adverse effects reported (most commonly nausea [6/65; 9%]) compared with 27 of 70 (39%; 95% CI 27% to 51%) in the ketamine group (most commonly disorientation [8/70; 11%]).

Conclusion
Intravenous morphine plus ketamine for out-of-hospital adult trauma patients provides analgesia superior to that of intravenous morphine alone but was associated with an increase in the rate of minor adverse effects.
Pour l'analgésie, La kétamine s'emploi à PETITES DOSES car c'est un coantalgique
30/04/2012
Sédation dissociative: La Kétamine
| Tags : kétamine
17/04/2012
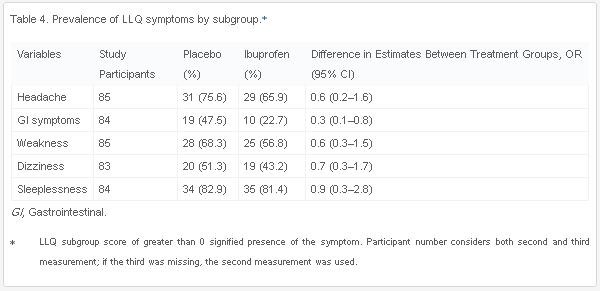
Ibuprofen pour le mal des montagnes
L'utilisation du diamox est reconnu pour la prévention du mal aigu des montagnes (Lire l'article). L'ibuprofen serait également efficace.
Ibuprofen Prevents Altitude Illness: A Randomized Controlled Trial for Prevention of Altitude Illness With Nonsteroidal Anti-inflammatories
Lipman GS et all. doi:10.1016/j.annemergmed.2012.01.019
Study objective
Acute mountain sickness occurs in more than 25% of the tens of millions of people who travel to high altitude each year. Previous studies on chemoprophylaxis with nonsteroidal anti-inflammatory drugs are limited in their ability to determine efficacy. We compare ibuprofen versus placebo in the prevention of acute mountain sickness incidence and severity on ascent from low to high altitude.
Methods
Healthy adult volunteers living at low altitude were randomized to ibuprofen 600 mg or placebo 3 times daily, starting 6 hours before ascent from 1,240 m (4,100 ft) to 3,810 m (12,570 ft) during July and August 2010 in the White Mountains of California. The main outcome measures were acute mountain sickness incidence and severity, measured by the Lake Louise Questionnaire acute mountain sickness score with a diagnosis of ≥ 3 with headache and 1 other symptom.
Results
Eighty-six participants completed the study; 44 (51%) received ibuprofen and 42 (49%) placebo. There were no differences in demographic characteristics between the 2 groups. Fewer participants in the ibuprofen group (43%) developed acute mountain sickness compared with those receiving placebo (69%) (odds ratio 0.3, 95% confidence interval 0.1 to 0.8; number needed to treat 3.9, 95% confidence interval 2 to 33). The acute mountain sickness severity was higher in the placebo group (4.4 [SD 2.6]) than individuals receiving ibuprofen (3.2 [SD 2.4]) (mean difference 0.9%; 95% confidence interval 0.3% to 3.0%)
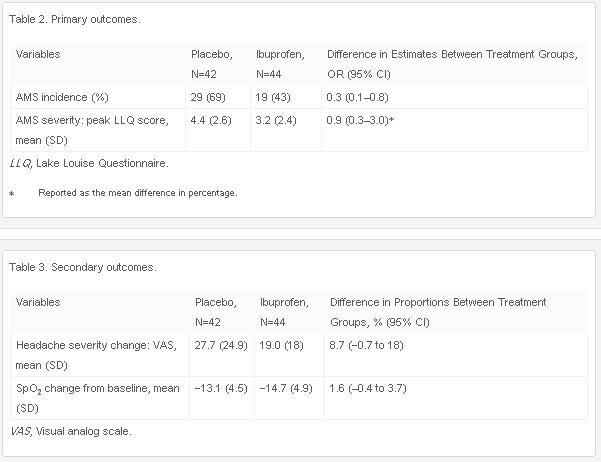
.Conclusion
Compared with placebo, ibuprofen was effective in reducing the incidence of acute mountain sickness.
24/12/2011
HEA, vraiment sûrs ?: Réponse début 2012 ?
Fluid Resuscitation with 6% Hydroxyethyl Starch (130/0.4) in Acutely Ill Patients: An Updated Systematic Review and Meta-Analysis
Gattas DJ et all. Anesth Analg 2012; 114:159–69
Une autre méta-analyse sur l'inocuité ou pas des solutions d'HEA 130 000/0,4 (Voluven]. Rien ne permet de conclure pour ou pas. Les auteurs estiment nécessaire de s'assurer de l'inocuité réele de ces produits par des travaux conduits de manière indépendante de l'industrie et sur une population plus large que celle de réanimation habituellement incluse. Ils mettent par ailleurs en avant le retrait récent de plusieurs publications portant sur la sécurité de ce type d'HEA. Il cite une étude intitulée Crystalloid versus Hydroxyethyl Starch Trial (CHEST) réalisée en australie portant sur l'analyse de la mortalité à 90 jours en comparant ce type de solutés à du salé isotonique qui devrait voir ses premiers résultats produits début 2012.

| Tags : remplissage, perfusion, choc
26/09/2011
Kétamine: Utilisation préhospitalière
| Tags : kétamine
30/08/2011
Exacyl: Bon aussi pour le blessé de guerre !
Une étude à paraître conduite par une équipe US a mis en évidence l'intérêt de l'acide tranexaminique.
----------------
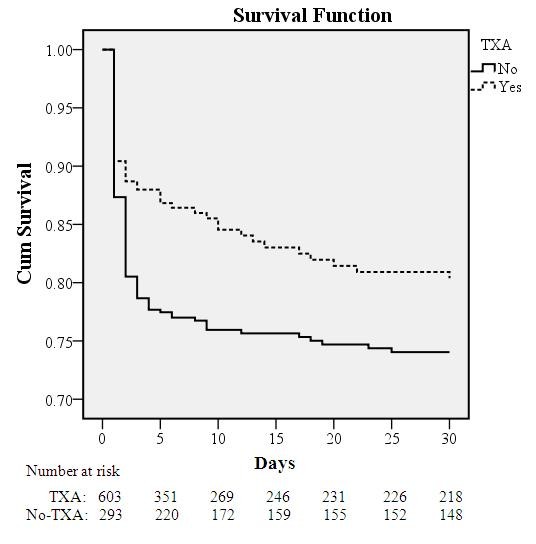
Tranexamic acid decreases mortality following wartime injury: the Military Application of Tranexamic acid in Trauma Emergency Resuscitation Study (MATTERS) MAJ Jonathan J. Morrison, MB ChB, MRCS, RAMC(V), LT COL (sel) Joseph J. Dubose, MD, USAF MC, COL Todd E. Rasmussen, MD, USAF MC, SURG CAPT Mark Midwinter, BMedSci, MD FRCS RN
http://archsurg.ama-assn.org/cgi/content/short/archsurg.2...
A recent registry-based study of combat injured troops receiving blood in Afghanistan (January 2009 - December 2010) at the Bastion Role 3 facility has demonstrated findings supportive of TXA use in this population. In a review of 896 combat casualties treated at Bastion over this time frame, 32.7% (N=293) received TXA (mean ± SD dose: 2.3 ± 1.3g) while 67.2% (N=603) did not receive TXA. In the overall cohort, the TXA group was more severely injured (ISS: 25.2±16.6 vs. 22.5±18.5; p<0.001), required more blood (11.8±12.1 vs. 9.8±13.1 pRBC units; p<0.001), and had a lower Glasgow Coma Score (7.3±5.5 vs. 10.5±5.5; p<0.001) and initial systolic blood pressure (112±29.1 vs. 122.5±30.3 mmHg), but also had a lower unadjusted mortality than the no-TXA group (17.4% vs. 23.9%; p=0.028). In the massive transfusion cohort (N=321; 24 hour transfusion: 21.9±14.7 pRBC; 19.1±13.3 FFP and 3.5±3.2 apheresis platelet units), mortality was also lower in the TXA (mean ± SD dose: 2.4 ± 1.4g) compared to the no-TXA group (14.4% vs. 28.1%; p=0.004). In a multivariate regression model, TXA use in the massive transfusion cohort was independently associated with survival (odds ratio: 7.28; 95% confidence interval: 3.02-17.32. For all patients requiring at least one unit of blood after combat injury, patients receiving TXA had higher rates of DVT (2.4% vs. 0.2%, p = 0.001) and PE (2.7% vs. 0.3%, p =0.001), but were also more likely to have injury patterns associated with higher risk of thromboembolic events ; including higher mean ISS (25 vs 23, p < 0.001), more severe extremity injuries (extremity AIS >=3 66.6% in TXA group, 47.3% non-TXA, p < 0.001), and more commonly GCS < or = 8 (63.3% vs. 35.6%, p < 0.001). These survival benefit findings associated with TXA use support the hypothesis that the use of this adjunct, in conjunction with component-based resuscitation following combat injury, is associated with improved survival. This association is most prominent in those requiring massive transfusion.
----------------
Exacyl 1g IV au mieux dans l'heure et pas après 3 heures après la blessure
16/08/2011
Guidelines for the prevention of infections associated with combat-related injuries: 2011 update
Une mise à jour du guide US de prévention des infections. A lire et à relire:
- Emballer les plaies avec des pansements STERILES.
- La céfazoline en première ligne avec comme alternative la clindamycine. Le détail ici.
- Il n'est pas utile d'ajouter de la pénicilline G pour la gangrène gazeuse.
- L'antibiothérapie doit être débutée au plus tôt, sur le terrain que si l'evasan est ou risque d'être tardive: Idéalement dans les 3 heures suivant la blessure.
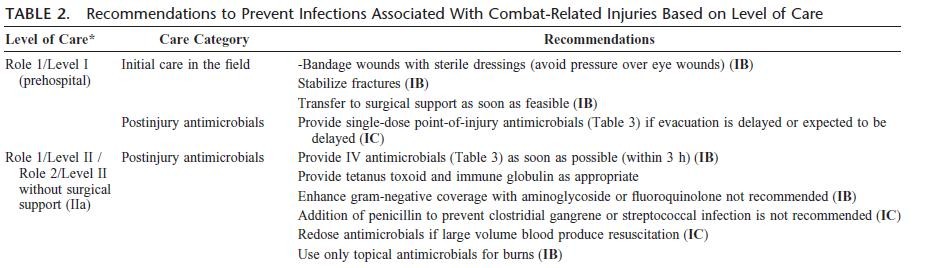
- L'irrigation à BASSE PRESSION des plaies par sérum salé ou eau de boisson est efficace. Le volume nécessare n'est pas connu. Un volume minimum de 3 l/j est avancé.
La synthèse est ici