23/10/2014
Pansements hémostatiques: Actualisation 2014
Review of New Topical Hemostatic Dressings for Combat Casualty Care
Benett BL et Al Mil Med. 2014 May;179(5):497-514
This review analyzes the new (2008-2013) hemostatic agents and dressings for enhanced efficacy in preclinical studies, and investigates supportive findings among case reports of effectiveness and safety in hospital and prehospital literature. A literature search was conducted using PubMed, National Library of Medicine using key words and phrases. The search revealed a total of 16 articles that fit the criteria established for third-generation hemostatic dressings. There were a total of 9 preclinical, 5 clinical, and 2 prehospital studies evaluated. Evaluation of these third- generation studies reveals that mucoadhesive (chitosan) dressings, particularly Celox Gauze and ChitoGauze, clearly show equal efficacy to Combat Gauze across many dependent variables. Chitosan-based products are ideal prehospital dressings because they are shown to work independently from the physiological clotting mechanisms. Many first-, second-, and third-generation chitosan-based dressings have been in use for years by the United States and other NATO militaries at the point of injury, and during tactical evacuation, in Operation Enduring Freedom and Operation Iraqi Freedom without reported complications or side effects. Based on the reported efficacy and long-term safety of chitosan-based products, increased use of Celox Gauze and ChitoGauze within the Department of Defense and civilian venues merits further consideration and open debate.
| Tags : hémorragie, pansement
14/09/2014
Plaie de l'abdomen: Comprimez avec le genou !
Abdominal aortic and iIiac artery compression following penetrating trauma: A study of feasibility
Douma et Al. Prehosp Disaster Med. 2014 Jun;29(3):299-302
Introduction
Penetrating junctional trauma is a leading cause of preventable death on the battlefield. Similarly challenging in civilian settings, exsanguination from the vessels of the abdomen, pelvis, and groin can occur in moments. Therefore, iliac artery or abdominal aortic compression has been recommended. Based on prior research, 120 lbs (54 kg) or 140 lbs (63 kg) of compression may be required to occlude these vessels, respectively. Whether most rescuers can generate this amount of compression is unknown.
Objective
To determine how many people in a convenience sample of 44 health care professionals can compress 120 lbs and 140 lbs.
Methods
This study simulated aortic and iliac artery compression. Consent was obtained from 44 clinicians (27 female; 17 male) from two large urban hospitals in Edmonton, Alberta, Canada. Participants compressed the abdominal model, which consisted of a medical scale and a 250 ml bag of saline, covered by a folded hospital blanket and placed on the ground. In random order, participants compressed a force they believed maintainable for 20 minutes (“maintainable effort”) and then a maximum force they could maintain for two minutes (“maximum effort”). Compression was also performed with a knee. Descriptive statistics were used to evaluate the data.
Results
Compression was directly proportional to the clinician's body weight. Participants compressed a mean of 55% of their body weight with two hands at a maintainable effort, and 69% at a maximum effort. At maintainable manual effort, participants compressed a mean of 86 lbs (39 kg). Sixteen percent could compress over 120 lbs, but none over 140 lbs. At maximum effort, participants compressed a mean of 108 lbs (48 kg). Thirty-four percent could compress greater than 120 lbs and 11% could compress greater than 140 lbs. Using a single knee, participants compressed a mean weight of 80% of their body weight with no difference between maintainable and maximum effort.
Conclusion
This work suggests that bimanual compression following penetrating junctional trauma is feasible. However, it is difficult, and is not likely achievable or sustainable by a majority of rescuers. Manual compression (used to temporize until device application and operative rescue) requires a large body mass. To maintain 140 lbs of compression (for example during a lengthy transport), participants needed to weigh 255 lbs (115 kg). Alternatively, they needed to weigh 203 lbs (92 kg) to be successful during brief periods. Knee compression may be preferable, especially for lower-weight rescuers.
| Tags : hémorragie
31/05/2014
Pansements hémostatiques: Utilité non démontrée
Haemostatic dressings in prehospital care
Hewitt Smith A. et Al. Emerg Med J 2013; 30:784–789
--------------------------------------------------------------
Une revue de littérature qui confirme que le bien fondé de l'emploi des pansements hémostatiques n'est pas si solide que cela. Pansement compressif et packing de plaie sont des valeurs sûres.
--------------------------------------------------------------
| Tags : pansement, hémorragie, massive bleeding control
07/04/2014
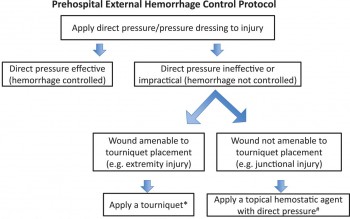
Le point sur le contrôle des hémorragies externes
An Evidence-based Prehospital Guideline for External Hemorrhage Control: American College of Surgeons Committee on Trauma
Bulger EM et Al. Prehosp Emerg Care. 2014 Apr-Jun;18(2):163-73.
Cet article fait le point à partir de données publiées sur les grands principes d'arrêt des hémorragies externes: Compression directe, garrot artériel en cas d'inefficacité, relatif faible niveau de preuves pour les pansements hémostatiques à utiliser néanmoins comme agent de packing de plaies, nécessité de poursuivre la recherche sur les dispositifs de compression jonctionnelle.
ATTENTION Il s'agit de préhospitalier CIVIL
Clic sur l'image pour accéder au document
| Tags : hémorragie, garrot
24/02/2014
Garrot abdominal: Il est efficace
Abdominal Aortic Tournique Use in Afghanistan
Anonymous. J Spec Oper Med. 2013 Summer;13(2):1-2.
La prise en charge des blessés de guerre a pour objectif essentiel d'obtenir l'arrêt des hémorragies le plus précocement possible. Parmi les dispositifs récemment proposés on trouve le garrot abdominal. On rapporte ici l'emploi couronné de succès d'un tel dispositif.

| Tags : garrot, hemorragie
18/02/2014
Electricité et hémorragie non compressible ?
Vasoconstriction by Electrical Stimulation: New Approach to Control of Non-Compressible Hemorrhage
Mandel Y et AL. Sci Rep. 2013; 3: 2111.
Non-compressible hemorrhage is the most common preventable cause of death on battlefield and in civilian traumatic injuries. We report the use of microsecond pulses of electric current to induce rapid constriction in femoral and mesenteric arteries and veins in rats. Electrically-induced vasoconstriction could be induced in seconds while blood vessels dilated back to their original size within minutes after stimulation. At higher settings, a blood clotting formed, leading to complete and permanent occlusion of the vessels. The latter regime dramatically decreased the bleeding rate in the injured femoral and mesenteric arteries, with a complete hemorrhage arrest achieved within seconds. The average blood loss from the treated femoral artery during the first minute after injury was about 7 times less than that of a non-treated control.
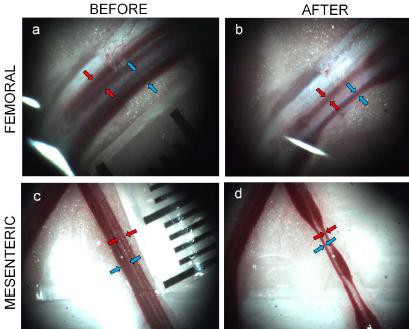
This new treatment modality offers a promising approach to non-damaging control of bleeding during surgery, and to efficient hemorrhage arrest in trauma patients
| Tags : hémorragie, jonctionnel
07/01/2014
Pansement hémostatique: Restons critiques !
An Evidence-Based Review of the Use of a Combat Gauze (QuikClot) for Hemorrhage Control
Gegel BT et Al. Am Surg. 2011 Feb;77(2):162-5.
_________________________________________________________________________
L'efficacité des pansements hémostatiques apparaît être une évidence. Ils sont utilisés de manière large sans véritables fondements scientiifiques prouvés. Une analyse critique s'impose, ce d'autant qu'il s'agit de produits onéreux et que l'industrie a bien façonné notre manière de raisonner. Cet article le rappelle.
_________________________________________________________________________
Trauma is a leading cause of morbidity and mortality. Uncontrolled hemorrhage related to the traumatic event is often the major cause of complications and death. The use of hemostatic agents may be one of the easiest and most effective methods of treating hemorrhage. The US military recommends a hemostatic combat gauze (QuikClot Combat Gauze) as the first-line hemostatic agent for use in treatment of severe hemorrhage. This review provides essential information for evidence-based use of this agent. The PICO (patient, intervention, comparison, outcome) question guiding this search for evidence was: Is QuikClot Combat Gauze, a hemostatic agent, effective and safe in controlling hemorrhage in trauma patients in the prehospital setting? The evidence appraised was a combination of lower-level human and animal research. It did not conclusively demonstrate that this combat gauze is an effective hemostatic agent for use in trauma patients, but the results are promising in supporting its use. The evidence does not describe serious side effects, exothermic reaction, and thromboemboli formation associated with other hemostatic agents. Further inves tigation to determine the effectiveness of hemostatic agents, specifically QuikClot Combat Gauze, in the management of trauma casualties in the prehospital setting is required. These should include large-scale, multicenter, prehospital randomized controlled trials.
| Tags : hémorragie, pansement
08/12/2013
Tourniquet abdominal: En théorie cela fonctionne
The Evaluation of an Abdominal Aortic Tourniquet for the Control of Pelvic and Lower Limb Hemorrhage
Taylor D. et Al.Mil Med. 2013;178(11):1196-201
Despite improved body armor, hemorrhage remains the leading cause of preventable death on the battlefield. Trauma to the junctional areas such as pelvis, groin, and axilla can be life threatening and difficult to manage. The Abdominal Aortic Tourniquet (AAT) is a prehospital device capable of preventing pelvic and proximal lower limb hemorrhage by means of external aortic compression. The aim of the study was to evaluate the efficacy of the AAT. Serving soldiers under 25 years old were recruited. Basic demographic data, height, weight, blood pressure, and abdominal girth were recorded. Doppler ultrasound was used to identify blood flow in the common femoral artery (CFA). The AAT was applied while the CFA flow was continuously monitored. The balloon was inflated until flow in the CFA ceased or the maximum pressure of the device was reached. A total of 16 soldiers were recruited. All participants tolerated the device. No complications were reported. Blood flow in the CFA was eliminated in 15 out of 16 participants. The one unsuccessful subject was above average height, weight, body mass index, and abdominal girth. This study shows the AAT to be effective in the control of blood flow in the pelvis and proximal lower limb and potentially lifesaving.
| Tags : hémorragie
24/11/2013
Garrot abdominal: Une paire de main et des bras musclés
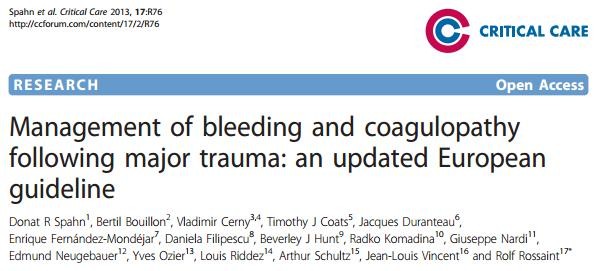
Temporization of Penetrating Abdominal-Pelvic Trauma With Manual External Aortic Compression: A Novel Case Report
Douma M et Al. Ann Emerg Med. 2013 Oct 23. pii: S0196-0644(13)01452-2
La prise en charge des traumatismes vasculaires de l'abdomen, du pelvis et des membres nécessite une intervention chirurgicale rapide. Il est dans ces cas nécessaire de tarir sinon de réduire le débit de saignement de telle sorte que le blessé arrive vivant dans la structure adaptée (1). Ceci est difficile quand les lésions ne sont pas ou difficilement garrotables notamment lors de traumatismes jonctionnels. Des équipements spécifiques ont été développé pour assurer une compression en amont des lésions et permettre de réduire ces débits de saignements. Ces dispositifs présenté par ailleurs (2, 3 , 4) n'ont pas encore fait leur preuve même si des rapports isolés en soulignent l'intérêt. Certains comme les pantalons antichocs sont considérés comme ayant peu d'indications du moins mal cernées (5) . Ces équipements sont rarement disponibles.
Pourtant la compression abdominale bi-manuelle est possible et en fait connue depuis longtemps notamment en obstétrique sous forme de compression utérine bi-manuelle (6, 7, 8).
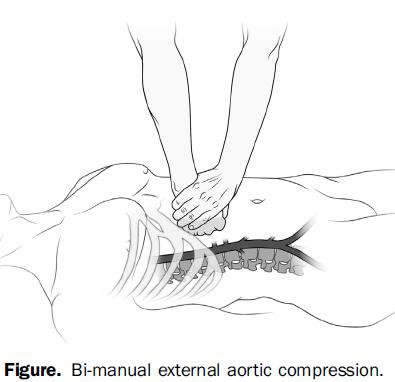
C'est ce qu'illustre le cas clinique présenté. Il existe bien sûr des facteurs limitant comme la corpulence aussi bien du blessé que du sauveteur. Il faut en effet exercer une pression abdominale de l'ordre de 40 kg pour occlure l'aorte abdominal (9).
| Tags : hémorragie, garrot
06/11/2013
Pansement compressif: Un nouveau venu
Il existe une grande variété de pansements compressifs. L'armée française utilise le pansement dit israélien de la société Persys Medical et le pansement Olaes modular bandage de la société TacMed Solutions. En plus des bandes de compression, d'autres dispositifs on fait leur apparition visant à contrôler les hémorragies par une compression plus proximale (le CROC, le tourniquet abdominal, le SAMTourniquet, le Junctional emergency treatment tool). Ces dispositifs ont recours à des dispositifs de compression. L'Aiwrap est un pansement compressif proche des pansements en dotation auquel est adjoint une vessie qui une fois gonflée va majorer de manière importante la compression sous le pansement. Son positionnement dans une gamme de produit reste à préciser.


| Tags : hémorragie, pansement
06/09/2013
Tourniquet abdominal: Compression axillaire ?

| Tags : tourniquet, hémorragie, jonctionnel
07/08/2013
Plasma: En préhospitalier AUSSI +++
Point-of-injury use of reconstituted freeze dried plasma as a resuscitative fluid: A special report for prehospital trauma care
Glassberg E. et All. J J Trauma Acute Care Surg. 2013;75(Suppl 2):S111YS111.
La prise en charge d'hémorrragie catastrophique en phase préhospitalière est particulièrement complexe. Ces dernières années la mise en place d'un réseau structuré de prise en charge, 'application de procédures spécifiques visant à arrêter les hémorragies au plus tôt, le recours à l'acide tranexaminique, la prévention des hypothermies et l'application d'une politique raisonnée de rénaimation/chirurgie ont constitué une grande avancée. Certaines nations ont équipé leurs vecteurs d'évacuations de concentrés érythrocytaires. Le maintien d'une coagulation optimale est un enjeu majeur. Pour cela existe, entre autres, le plasma lyophilisé. Les forces armées israéliennes militent pour l'emploi de ce type de solutions en phase préhospitalière
| Tags : coagulopathie, hémorragie
16/07/2013
Consensus statement of the ESICM task force on colloid volume therapy in critically ill patients
We recommend not to use HES with molecular weight C200 kDa and/or degree of substitution[0.4 in patients with severe sepsis or risk of acute kidney injury and suggest not to use 6% HES130/0.4 or gelatin in these populations. We recommend not to use colloids in patients with head injury and not to administer gelatins and HES in organ donors. We suggest not to use hyperoncotic solutions for fluid resuscitation. We conclude and recommend that any new colloid should be introduced into clinical practice only after its patient-important safety parameters are established.
| Tags : hémorragie, traumatologie
Management of bleeding and coagulopathy following major trauma: an updated European guideline
| Tags : hémorragie, traumatologie
04/07/2013
Hémostase: L'émergence des nanoparticules ?
Nano hemostat solution: immediate hemostasis at the nanoscale
Ellis-Behnke RG et all. Nanomedicine: Nanotechnology, Biology, and Medicine 2 (2006) 207 – 215
--------------------------------------------------------------------------------------
Hemostasis is a major problem in surgical procedures and after major trauma. There are few effective methods to stop bleeding without causing secondary damage. We used a self-assembling peptide that establishes a nanofiber barrier to achieve complete hemostasis immediately when applied directly to a wound in the brain, spinal cord, femoral artery, liver, or skin of mammals. This novel therapy stops bleeding without the use of pressure, cauterization, vasoconstriction, coagulation, or cross-linked adhesives. The self-assembling solution is nontoxic and nonimmunogenic, and the breakdown products are amino acids, which are tissue building blocks that can be used to repair the site of injury. Here we report the first use of nanotechnology to achieve complete hemostasis in less than 15 seconds, hich could fundamentally change how much blood is needed during surgery of the future.
--------------------------------------------------------------------------------------
Dans ce modèle une hémostase obtenue en moins de 15 secondes par un mécanisme peu évident:
1. ["First, we know that the hemostasis is not explainable by clotting. Blood clots are produced after injury, but do not begin to form until 1 to 2 minutes have elapsed, depending upon the status and coagulation history of the patient"]
2. ["the electron micrographs show no evidence of platelet aggregation at the interface of the material and wound site"]
3. ["We believe this tight contact is crucial to the hemostatic action because of the size of the self-assembling peptide units."]
| Tags : hémorragie
02/07/2013
Croc axillaire:En théorie, c'est possible
Technique of axillary use of a Combat Ready Clamp to stop junctional bleeding
Kragh JF et All. http://dx.doi.org/10.1016/j.ajem.2013.02.027
Bien que le Croc ne soit validé que les plaies de l'aine, son emploi au membre supérieur est possible.
Enlever la cupule et appliquer la barre de compression parallèle à la clavicule. Le serrage compotre en moyenne 5 tours.
| Tags : hémorragie
02/06/2013
Hémorragies jonctionnelles: Comprimer le pelvis
UK Combat-Related Pelvic Junctional Vascular Injuries 2008-2011: Implications for Future Intervention.
Walker NM et All. - Bone Joint Journal (2013) vol. 95-B no. SUPP 8 13
---------------------------------------------------------------------------------------
L'arrêt d'une hémorragie jonctionnelle est un enjeu majeur. Plusieurs dispositifs ont été récemment proposés. Il semble que la grande majorité des lésions observées se situent au dessus du ligament inguinal rendant ainsi l'efficacité de dispositif comme le CRoC limité. Le tourniquet abdominal ou le sam junctionnal tourniquet paraissent ainsi au moins théoriquement un meilleur choix si toutefois ils permettent une compression suffisante.
---------------------------------------------------------------------------------------
In a recent publication, 4.6% of 6450 Coalition deaths over ten years were reported to be due to junctional bleeding. The authors suggested that some of these deaths could have been avoided with a junctional hemorrhage control device.
Prospectively collected data on all injuries sustained in Afghanistan by UK military personnel over a 2 year period were reviewed. All fatalities with significant pelvic injuries were identified and analysed, and the cause of death established.
Significant upper thigh, groin or pelvic injuries were recorded in 124 casualties, of which 92 died. Pelvic injury was the cause of death in 42; only 1 casualty was identified where death was at least in part due to a vascular injury below the inguinal ligament, not controlled by a tourniquet, representing <1% of all deaths. Twenty one deaths were due to vascular injury between the aortic bifurcation and the inguinal ligament, of which 4 survived to a medical facility.
Some potentially survivable deaths due to exsanguination may be amenable to more proximal vascular control. We cannot substantiate previous conclusions that this can be achieved through use of a groin junctional tourniquet. There may be a role for more proximal vascular control of pelvic bleeding.
| Tags : tourniquet, hémorragie, jonctionnel
20/04/2013
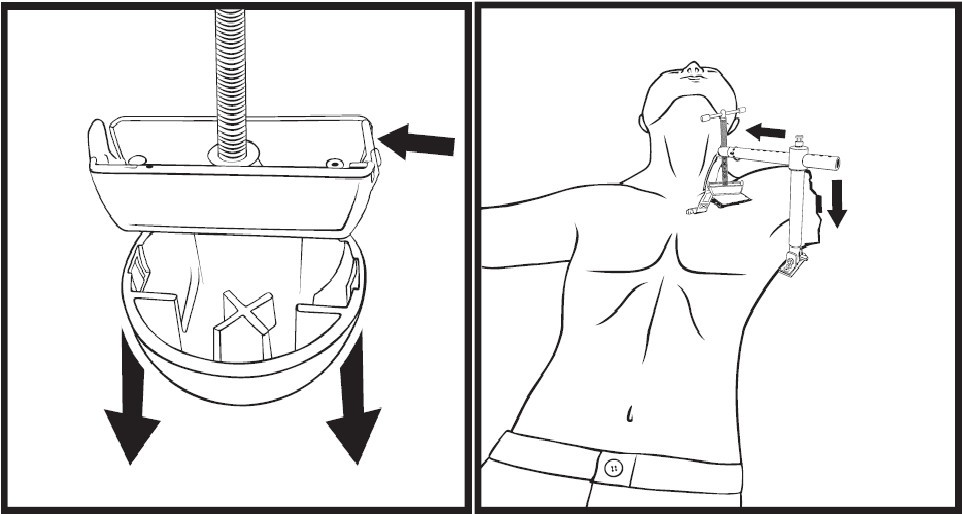
Hémorragie jonctionnelle: Un nouveau dispositif de compression
La prise en charge des hémorragies jonctionnelles est un des enjeux actuels de la chirurgie de guerre. Réaliser une compression artérielle fémorale peut être obtenu manuellement ou bien à l'aide de dispositifs mécaniques. L'utilisation du Combat Ready Clamp (CRoC) fait partie de la doctrine actuelle du TCCC américain. Un produit similaire est proposé: Le Junctionnal Emergency Treatment Tool (JETT). L'intérêt de ce type de dispositifs ne parait pas devoir être limité au préhospitalier. Ils sont en effet utilisés de manière courante à l'hôpital notamment pour comprimer les régions fémorales lors du retrait des dispositifs artériels fémoraux (femostop). Un troisième dispositif compressif vient compléter l'offre: Le SAM junctionnal tourniquet dont l'usage semble plus simple et qui offre surtout l'avantage de réaliser une stabilisation pelvienne. (voir ici sa validation sur cadavre)
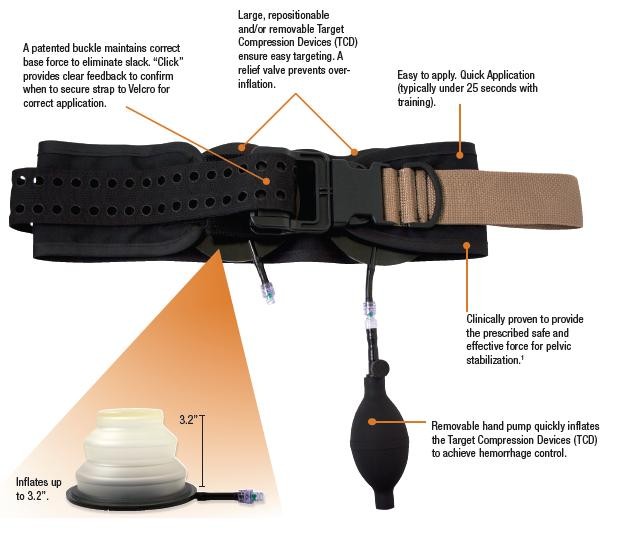
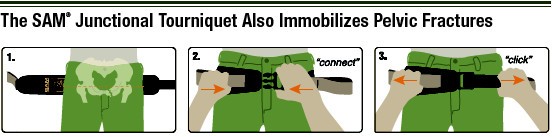
Cependant malgré tout leur intérêt potentiel aucun de ces produits n'a été vraiment validé
| Tags : hémorragie, jonctionnel, garrot
21/02/2013
Pour la coagulation: HEA de haut PM pas bon ?
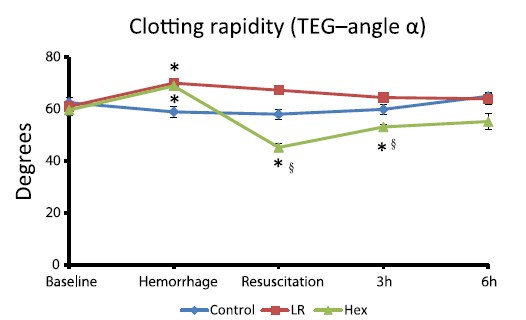
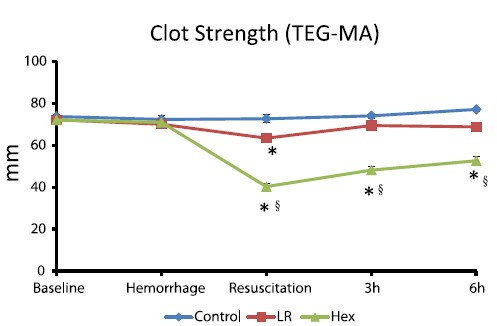
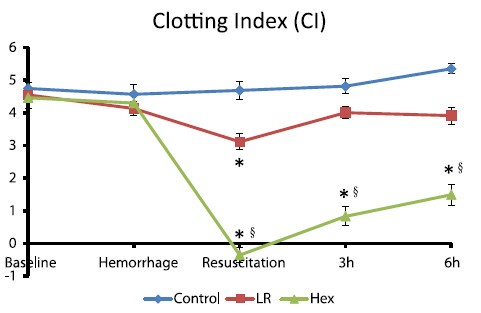
Comparisons of lactated Ringer’s and Hextend resuscitation on hemodynamics and coagulation following femur injury and severe hemorrhage in pigs
Wenjun Z et all J Trauma Acute Care Surg. 2013;74: 732-740
After traumatic hemorrhage, coagulation function was restored within 6 hours with LR resuscitation but not with Hextend. The lack of recovery after Hextend is likely caused by greater hemodilution and possible effects of starches on coagulation substrates and further documents the need to restrict the use of high-molecular-weight starch in resuscitation fluids for bleeding casualties.
On rappelle que l'Hextend est un HEA 670/0.75 et que le voluven est un HEA 130/0,4 dont les effets sur la coagulation sont réputées étant moindres.
| Tags : coagulopathie, remplissage, hémorragie
02/12/2012
Hémostase et transfusion par A. Godier IAR IDF

CLIC sur le logo pour accéder au cours
| Tags : hémorragie