08/06/2022
Trauma Prehospitalier: Aides
| Tags : traumatologie
07/09/2013
Causes de DC évitables: Actualisation UK
Identifying future ‘unexpected’ survivors: a retrospective cohort study of fatal injury patterns in victims of improvised explosive devices
To identify potentially fatal injury patterns in explosive blast fatalities in order to focus research and mitigation strategies, to further improve survival rates from blast trauma.
DESIGN:
Retrospective cohort study.
PARTICIPANTS:
UK military personnel killed by improvised explosive device (IED) blasts in Afghanistan, November 2007-August 2010.
SETTING:
UK military deployment, through NATO, in support of the International Security Assistance Force (ISAF) mission in Afghanistan.
DATA SOURCES:
UK military postmortem CT records, UK Joint Theatre Trauma Registry and associated incident data.
MAIN OUTCOME MEASURES:
Potentially fatal injuries attributable to IEDs.
RESULTS:
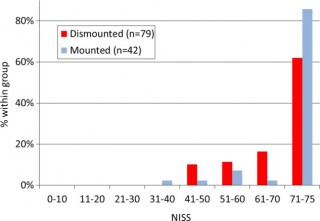
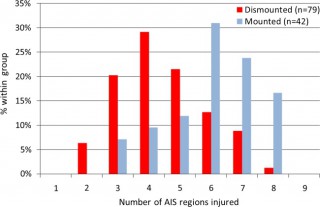
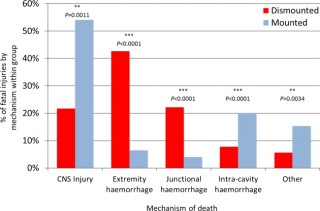
We identified 121 cases, 42 mounted (in-vehicle) and 79 dismounted (on foot), at a point of wounding. There were 354 potentially fatalinjuries in total. Leading causes of death were traumatic brain injury (50%, 62/124 fatal injuries), followed by intracavity haemorrhage (20.2%, 25/124) in the mounted group, and extremity haemorrhage (42.6%, 98/230 fatal injuries), junctional haemorrhage (22.2%, 51/230 fatal injuries) and traumatic brain injury (18.7%, 43/230 fatal injuries) in the dismounted group.
CONCLUSIONS:
Head trauma severity in both mounted and dismounted IED fatalities indicated prevention and mitigation as the most effective strategies to decrease resultant mortality. Two-thirds of dismounted fatalities had haemorrhage implicated as a cause of death that may have been anatomically amenable to prehospital intervention. One-fifth of the mounted fatalities had haemorrhagic trauma which currently could only be addressed surgically. Maintaining the drive to improve all haemostatic techniques for blast casualties, from point of wounding to definitive surgical proximal vascular control, alongside the development and application of novel haemostatic interventions could yield a significant survival benefit. Prospective studies in this field are indicated.
Cette publication est très importante car elle insiste sur l'absolue nécessité de poursuivre les efforts en vue de prévenir le trauma aussi bien en matière de protection balistique, de réduction des délais de transports pour permettre la prise en charge d'hémorragie intra-cavitaires et l'aspect fondamental d'arrêter toutes les hémorragies sur le terrain notamment pas la mise en oeuvre d'une nouvelle catégorie de garrots pour les hémorragies jonctionnelles (voir 1, 2, 3, 4, 5, 6)
Les morts par IED sont plus sévèrement atteints dans un véhicule qu'à pied.
58% des Décès sont liés à plus de 2 causes potentiellement évitables
Les causes de décès ne sont pas les mêmes en combat à pied ou en véhicule
| Tags : balistique, blast, traumatologie, explosion, jonctionnel
16/07/2013
Consensus statement of the ESICM task force on colloid volume therapy in critically ill patients
We recommend not to use HES with molecular weight C200 kDa and/or degree of substitution[0.4 in patients with severe sepsis or risk of acute kidney injury and suggest not to use 6% HES130/0.4 or gelatin in these populations. We recommend not to use colloids in patients with head injury and not to administer gelatins and HES in organ donors. We suggest not to use hyperoncotic solutions for fluid resuscitation. We conclude and recommend that any new colloid should be introduced into clinical practice only after its patient-important safety parameters are established.
| Tags : hémorragie, traumatologie
Management of bleeding and coagulopathy following major trauma: an updated European guideline
| Tags : hémorragie, traumatologie
29/06/2013
Blessés thoraciques: Données UK
The UK military experience of thoracic injury in the wars in Iraq and Afghanistan
Poon H. et All. Injury. 2013 Feb 20. pii: S0020-1383(13)00073-9.
INTRODUCTION:
Thoracic injury during warfare is associated with a high incidence of morbidity and mortality. This study examines the pattern and mortality of thoracic wounding in the counter-insurgency conflicts of Iraq and Afghanistan, and outlines the operative and decision making skills required by the modern military surgeon in the deployed hospital setting to manage these injuries.
METHODS:
The UK Joint Theatre Trauma Registry was searched between 2003 and 2011 to identify all patients who sustained battle-related thoracic injuries admitted to a UK Field Hospital (Role 3). All UK soldiers, coalition forces and local civilians were included.
RESULTS:
During the study period 7856 patients were admitted because of trauma, 826 (10.5%) of whom had thoracic injury. Thoracic injury-related mortality was 118/826 (14.3%). There were no differences in gender, age, coalition status and mechanism of injury between survivors and non-survivors. Survivors had a significantly higher GCS, Revised Trauma Score and systolic blood pressure on admission to a Role 3 facility. Multivariable regression analysis identified admission systolic blood pressure less than 90, severe head or abdominal injury and cardiac arrest as independent predictors of mortality.
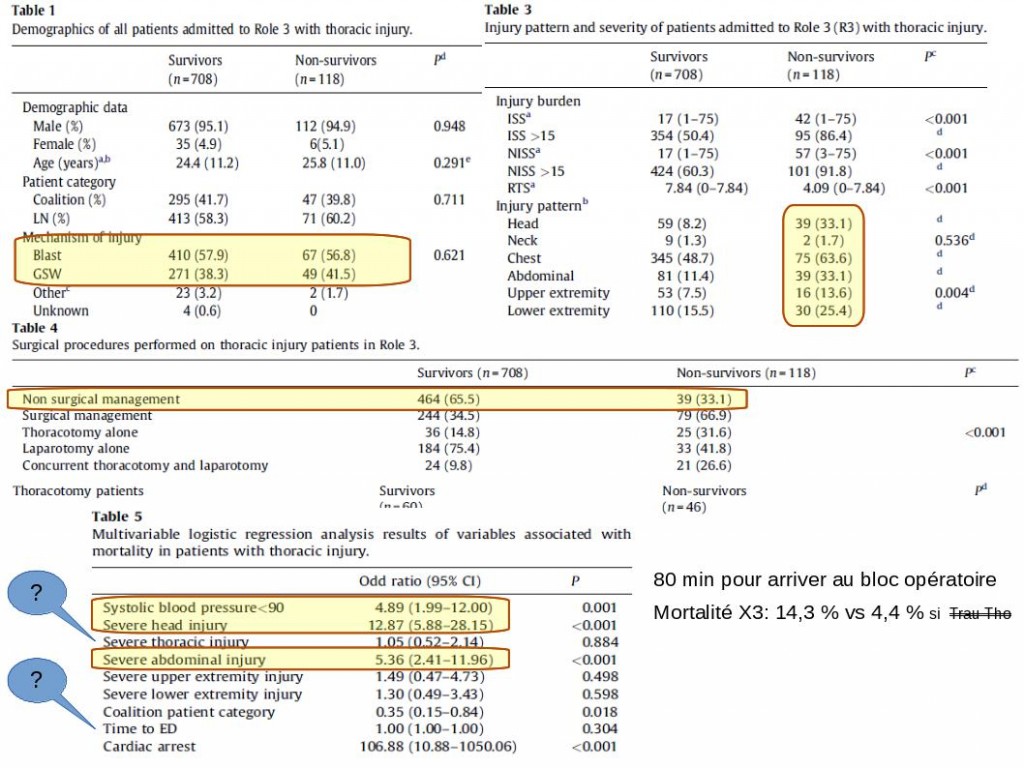
CONCLUSIONS:
Blast is the main mechanism of thoracic wounding in the recent conflicts in Iraq and Afghanistan. Thoracic trauma in association with severe head or abdominal injuries are predictors of mortality, rather than thoracic injury alone. Deploying surgeons require training in thoracic surgery in order to be able to manage patients appropriately at Role 3.
Commentaires
La plupart des traumatisés ne nécessite pas de chirurgie. Les survivants arrivent plus vite mais il ne semble pas qu'un délai un peu plus long soit associé avec une surmortalité. La gravité du traumatisme thoracique n'apparait pas être lié avec la mortalité. il existeune amélioration du pronostic rapporté à l'amélioration de la prise en charge globale.
| Tags : traumatologie, thorax
01/05/2012
Military medicine in the 21st century: pushing the boundaries of combat casualty care

| Tags : traumatologie
13/12/2009
Lien vers quelques cours de traumatologie
| Tags : traumatologie, cours en ligne