10/03/2019
Garrot jonctionnel: Pas si performant que cela !
Comparison of Three Junctional Tourniquets Using a Randomized Trial Design.
BACKGROUND:
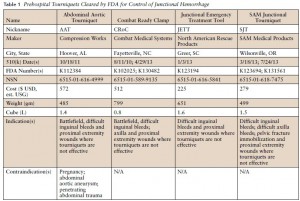
Hemorrhage remains a leading cause of death in both civilian and military settings. Of preventable deaths from hemorrhage, a significant portion occurs from junctional wounds that are not amenable to traditional extremity tourniquets. Junctional tourniquets (JTQs) can potentially provide hemorrhage control by compressing the arteries at the junction of the trunk and extremities. The FDA has cleared 3 JTQ products: The Combat Ready Clamp (CRoC®), the Junctional Emergency Treatment Tool (JETT™), and the SAM® JunctionalTourniquet (SJT). However, little is known regarding which of these JTQs is superior in application time, effectiveness in pulse elimination, effectiveness during transport, and user preference.
METHODS:
Active duty corpsmen (N = 49) were given standardized instruction and hands-on training with the CRoC®, JETT™, and SJT, then sequentially applied each JTQ unilaterally to a fellow study participant in a randomized order. Pulse elimination was determined by Doppler ultrasound at the dorsalis pedis immediately then reevaluated after a short transport. User preference data were collected following testing. Data were analyzed using repeated measures ANOVA and non-parametric statistics at p < 0.05.
RESULTS:
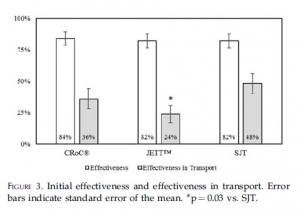
The CRoC® was significantly slower in application time than the JETT™ and SJT. Effectiveness was similar for CRoC®, JETT™, and SJT. Effectiveness during transport was significantly higher for SJT than for the JETT™, but no JTQ performed well during transport (24-48% effectiveness).
SJT ranked first in perceived ease of use, stability, and reliability, and in user trust and overall preference. Participants provided cogent suggestions for product improvement.
CONCLUSIONS:
All JTQ devices performed poorly during transport. Combined, present findings highlight the potential of JTQ products for saving lives threatened by junctional wounds, but also highlight the need for specific product improvements towards fostering JTQ performance in patient transport.
| Tags : jonctionnel
01/03/2018
Trauma jonctionnels: Une revue
Clic sur l'image pour accéder au document
| Tags : jonctionnel, hémorragie
02/07/2015
Hémorragie jonctionnelle: Croc ou Sam Tourniquet ?
| Tags : jonctionnel
31/10/2014
Garrot jonctionnel: CROC et SAM ?
Testing of junctional tourniquets by military medics to control simulated groin hemorrhage.
Kragh JF et Al. J Spec Oper Med. 2014 Fall;14(3):58-63.
Ce qui est certain, c'est ce qui est écrit sur cette image
Difficile d'avoir une idée précise sur les performances relatives des matériels proposés par les industriels. Ce qui suit éclaire un peu.
BACKGROUND:
Junctional hemorrhage is a common cause of death on the battlefield, but there is no documented direct comparison for the use of junctional tourniquet models by US medics. The purpose of this testing is to assess military medic experience with the use of junctional tourniquets in simulated out-of-hospital trauma care.
METHODS:
Nine medics (seven men and two women) used four different junctional tourniquets: Combat Ready Clamp™ (CRoC™; http://www.combatmedicalsystems.com), Abdominal Aortic and Junctional Tourniquet™ (AAJT™; http://www.compressionworks.net), Junctional Emergency Treatment Tool (JETT™; http://www.narescue .com), and SAM Junctional Tourniquet® (SJT®; http:// www.sammedical.com/products). These medics also acted as simulated casualties. Effectiveness percentages, as measured by stopped distal pulse by Doppler auscultation, and time to effectiveness were recorded in two tests per tourniquet (72 total tests). Tourniquet users ranked their preference of model by answering the question: "If you had to go to war today and you could only choose one, which tourniquet would you choose to bring?"
RESULTS:
All tourniquets used were safe under the conditions of this study. Both the SJT and the CRoC had high effectiveness percentages; their rate difference was not statistically significant. The SJT and the CRoC had fast times to effectiveness; their time difference was not statistically significant. Users preferred the SJT and the CRoC; their ranked difference was not statistically significant.
CONCLUSION:
The SJT and the CRoC were equally effective and fast and were preferred by the participants
| Tags : jonctionnel
14/04/2014
Tourniquet jonctionnel: Réflexions US
Management of Junctional Hemorrhage in Tactical Combat Casualty Care: TCCC Guidelines–Proposed Change 13-03
Kotwal RS et Al. J Spec Oper Med. 2013 Winter;13(4):85-93.
Clic sur l'image pour accéder au document
L'industrie nous propose des "garrots jonctionnels". Difficile de se faire une idée précise. Les US ont intégré le CRoC au TCCC. Cependant ce dispositif n'est pas si simple à monter. Cet article offre une lecture intéressante sur le sujet. Le tourniquet abdominal ne doit pas être appliqué plus d'une heure. Les autres le peuvent pour une durée maximum de 4 heures. Enfin le Sam Junctional Tourniquet est homologué par la FDA en tant que ceinture pelvienne.
| Tags : jonctionnel
18/02/2014
Electricité et hémorragie non compressible ?
Vasoconstriction by Electrical Stimulation: New Approach to Control of Non-Compressible Hemorrhage
Mandel Y et AL. Sci Rep. 2013; 3: 2111.
Non-compressible hemorrhage is the most common preventable cause of death on battlefield and in civilian traumatic injuries. We report the use of microsecond pulses of electric current to induce rapid constriction in femoral and mesenteric arteries and veins in rats. Electrically-induced vasoconstriction could be induced in seconds while blood vessels dilated back to their original size within minutes after stimulation. At higher settings, a blood clotting formed, leading to complete and permanent occlusion of the vessels. The latter regime dramatically decreased the bleeding rate in the injured femoral and mesenteric arteries, with a complete hemorrhage arrest achieved within seconds. The average blood loss from the treated femoral artery during the first minute after injury was about 7 times less than that of a non-treated control.
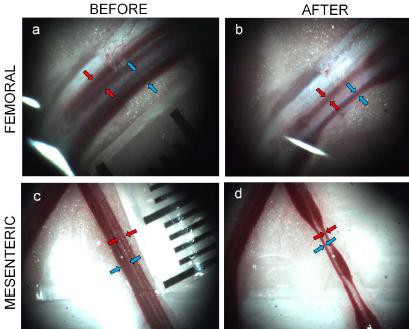
This new treatment modality offers a promising approach to non-damaging control of bleeding during surgery, and to efficient hemorrhage arrest in trauma patients
| Tags : hémorragie, jonctionnel
07/09/2013
Causes de DC évitables: Actualisation UK
Identifying future ‘unexpected’ survivors: a retrospective cohort study of fatal injury patterns in victims of improvised explosive devices
To identify potentially fatal injury patterns in explosive blast fatalities in order to focus research and mitigation strategies, to further improve survival rates from blast trauma.
DESIGN:
Retrospective cohort study.
PARTICIPANTS:
UK military personnel killed by improvised explosive device (IED) blasts in Afghanistan, November 2007-August 2010.
SETTING:
UK military deployment, through NATO, in support of the International Security Assistance Force (ISAF) mission in Afghanistan.
DATA SOURCES:
UK military postmortem CT records, UK Joint Theatre Trauma Registry and associated incident data.
MAIN OUTCOME MEASURES:
Potentially fatal injuries attributable to IEDs.
RESULTS:
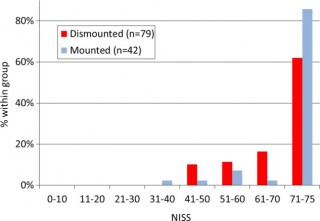
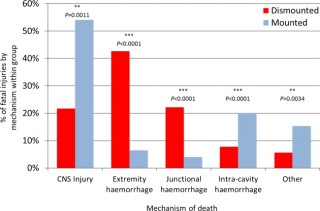
We identified 121 cases, 42 mounted (in-vehicle) and 79 dismounted (on foot), at a point of wounding. There were 354 potentially fatalinjuries in total. Leading causes of death were traumatic brain injury (50%, 62/124 fatal injuries), followed by intracavity haemorrhage (20.2%, 25/124) in the mounted group, and extremity haemorrhage (42.6%, 98/230 fatal injuries), junctional haemorrhage (22.2%, 51/230 fatal injuries) and traumatic brain injury (18.7%, 43/230 fatal injuries) in the dismounted group.
CONCLUSIONS:
Head trauma severity in both mounted and dismounted IED fatalities indicated prevention and mitigation as the most effective strategies to decrease resultant mortality. Two-thirds of dismounted fatalities had haemorrhage implicated as a cause of death that may have been anatomically amenable to prehospital intervention. One-fifth of the mounted fatalities had haemorrhagic trauma which currently could only be addressed surgically. Maintaining the drive to improve all haemostatic techniques for blast casualties, from point of wounding to definitive surgical proximal vascular control, alongside the development and application of novel haemostatic interventions could yield a significant survival benefit. Prospective studies in this field are indicated.
Cette publication est très importante car elle insiste sur l'absolue nécessité de poursuivre les efforts en vue de prévenir le trauma aussi bien en matière de protection balistique, de réduction des délais de transports pour permettre la prise en charge d'hémorragie intra-cavitaires et l'aspect fondamental d'arrêter toutes les hémorragies sur le terrain notamment pas la mise en oeuvre d'une nouvelle catégorie de garrots pour les hémorragies jonctionnelles (voir 1, 2, 3, 4, 5, 6)
Les morts par IED sont plus sévèrement atteints dans un véhicule qu'à pied.
58% des Décès sont liés à plus de 2 causes potentiellement évitables
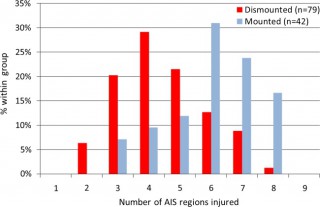
Les causes de décès ne sont pas les mêmes en combat à pied ou en véhicule
| Tags : balistique, blast, traumatologie, explosion, jonctionnel
06/09/2013
Tourniquet abdominal: Compression axillaire ?

| Tags : tourniquet, hémorragie, jonctionnel
05/07/2013
Garrot: Une nouvelle ère ?
New Tourniquet Device Concepts for Battlefield Hemorrhage Control
Kragh JF et all.US Army Med Dep J. 2011 Apr-Jun:38-48.
Ground:
Given the recent success of emergency tourniquets, limb exsanguination is no longer the most common cause of preventable death on the battlefield; hemorrhage amenable to truncal tourniquets now is. The purpose of the present study is to discuss the gaps today in battlefield hemorrhage control and candidate solutions in order to stimulate the advancement of prehospital combat casualty care.
Methods:
A literature review, a market survey of candidate devices, a request for devices, and an analysis of the current situation regarding battlefield hemorrhage control were performed.
Results:
Hemorrhage control for wounds in the junction between the trunk and the limbs and neck is a care gap in the current war, and, of these, the pelvic (including buttock and groin proximal to the inguinal ligament) area is the most common. Historical and recent reports give background information indicating that truncal tourniquets are plausible devices for controlling junctional hemorrhage on the battlefield. A request for candidate devices yielded few prototypes, only one of which was approved by the US Food and Drug Administration.
Conclusions:
In order to solve the now most common cause of preventable death on the battlefield, junctional hemorrhage from the pelvic area, the planned approach is a systematic review of research, device and model development, and the fielding of a good device with appropriate training and doctrine.
| Tags : jonctionnel, tourniquet
02/06/2013
Hémorragies jonctionnelles: Comprimer le pelvis
UK Combat-Related Pelvic Junctional Vascular Injuries 2008-2011: Implications for Future Intervention.
Walker NM et All. - Bone Joint Journal (2013) vol. 95-B no. SUPP 8 13
---------------------------------------------------------------------------------------
L'arrêt d'une hémorragie jonctionnelle est un enjeu majeur. Plusieurs dispositifs ont été récemment proposés. Il semble que la grande majorité des lésions observées se situent au dessus du ligament inguinal rendant ainsi l'efficacité de dispositif comme le CRoC limité. Le tourniquet abdominal ou le sam junctionnal tourniquet paraissent ainsi au moins théoriquement un meilleur choix si toutefois ils permettent une compression suffisante.
---------------------------------------------------------------------------------------
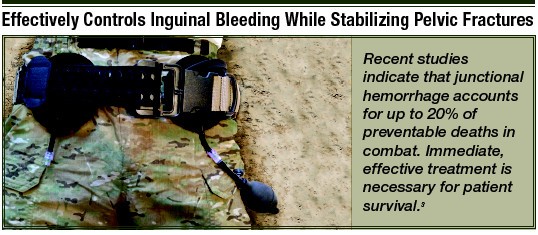
In a recent publication, 4.6% of 6450 Coalition deaths over ten years were reported to be due to junctional bleeding. The authors suggested that some of these deaths could have been avoided with a junctional hemorrhage control device.
Prospectively collected data on all injuries sustained in Afghanistan by UK military personnel over a 2 year period were reviewed. All fatalities with significant pelvic injuries were identified and analysed, and the cause of death established.
Significant upper thigh, groin or pelvic injuries were recorded in 124 casualties, of which 92 died. Pelvic injury was the cause of death in 42; only 1 casualty was identified where death was at least in part due to a vascular injury below the inguinal ligament, not controlled by a tourniquet, representing <1% of all deaths. Twenty one deaths were due to vascular injury between the aortic bifurcation and the inguinal ligament, of which 4 survived to a medical facility.
Some potentially survivable deaths due to exsanguination may be amenable to more proximal vascular control. We cannot substantiate previous conclusions that this can be achieved through use of a groin junctional tourniquet. There may be a role for more proximal vascular control of pelvic bleeding.
| Tags : tourniquet, hémorragie, jonctionnel
20/04/2013
Hémorragie jonctionnelle: Un nouveau dispositif de compression
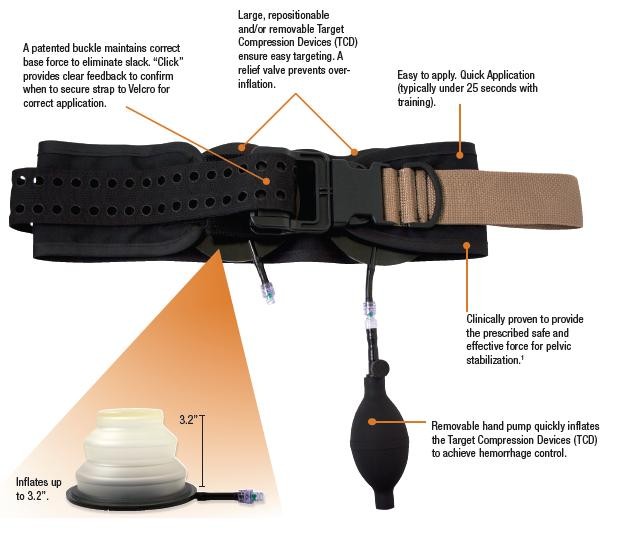
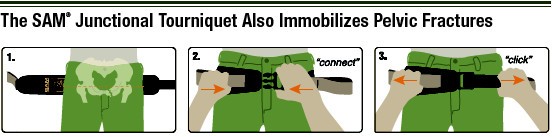
La prise en charge des hémorragies jonctionnelles est un des enjeux actuels de la chirurgie de guerre. Réaliser une compression artérielle fémorale peut être obtenu manuellement ou bien à l'aide de dispositifs mécaniques. L'utilisation du Combat Ready Clamp (CRoC) fait partie de la doctrine actuelle du TCCC américain. Un produit similaire est proposé: Le Junctionnal Emergency Treatment Tool (JETT). L'intérêt de ce type de dispositifs ne parait pas devoir être limité au préhospitalier. Ils sont en effet utilisés de manière courante à l'hôpital notamment pour comprimer les régions fémorales lors du retrait des dispositifs artériels fémoraux (femostop). Un troisième dispositif compressif vient compléter l'offre: Le SAM junctionnal tourniquet dont l'usage semble plus simple et qui offre surtout l'avantage de réaliser une stabilisation pelvienne. (voir ici sa validation sur cadavre)
Cependant malgré tout leur intérêt potentiel aucun de ces produits n'a été vraiment validé
| Tags : hémorragie, jonctionnel, garrot
13/12/2011
25 recommandations UK pour les traumas jonctionnels
http://www.medicalsca.com/files/emf_parker_junctional_tra...
Une affaire d'équipe pour une prise en charge "aggressive" qu'il faut avoir réfléchi AVANT
| Tags : jonctionnel, hémorragie