02/12/2012
Choc hémorragique par D. Journois IAR IDF
CLIC sur le logo pour visualiser le cours
| Tags : choc, hémorragie, remplissage
23/09/2012
Facteur VIIa: Intérêt pas prouvé !
Use of recombinant factor VIIA for control of combat-related haemorrhage.
Woodruff SI et all. Emerg Med J 2010;27:2 121-124
Ce travail met en exergue que le recours au FVIIa n'a pas d'intérêt prouvé en cas de prise en charge de traumatismes pénétrants. Ceci est d'autant plus vrai qu'il est fait alors qu'une coagulopathie sévère est installée (The utility of recombinant factor VIIa as a last resort in trauma. Mamtani R. et all. World Journal of Emergency Surgery 2012, 7(Suppl 1):S7)
----------------------------------------------
Background
Recombinant activated human coagulation factor VII (rFVIIa), an intravascular strategy to promote clotting, is being used as an adjunct to surgical control of bleeding in combat trauma patients.
Objective
To describe the initial experiences with rFVIIa administered to combat casualties at US Navy-Marine Corps medical treatment facilities in Iraq, and to comparesurvival outcomes of those treated with rFVIIa to controls not receiving rFVIIa.
Methods
Medical encounter data from the US Navy-Marine Corps Combat Trauma Registry were retrospectively reviewed to identify all battle-injured patients documented as having received rFVIIa during the period May 2004 to January 2006 of Operation Iraqi Freedom. Available clinical and injury related data are presented to characterise the patients. To assess effects of rFVIIa on survival outcomes, rFVIIa cases were matched to controls on injury severity and age.
Results
22 battle-injured patients from the Combat Trauma Registry received rFVIIa. Primarily young US Marines, these patients typically had penetrating injuries from improvised explosive devices and gunshot wounds. Injuries were often abdominal. The average dose used was similar to that reported in another study of civilian trauma patients, although dosing varies widely in the existing experimental and anecdotal literature. Over two-thirds (68%) of the rFVIIa patients surviveddan identical outcome seen for a matched control group of 22 patients.
Conclusions
Survival of seriously injured combat casualties was good, although identical to that of a control group. Methodological limitations of this retrospective study preclude making firm conclusions about the effectiveness of rFVIIa. Future controlled studies are needed for safety and efficacy testing of rFVIIa in combat trauma patients.
----------------------------------------------
| Tags : hémorragie, coagulopathie
08/09/2012
Moins remplir: Mieux ? Oui, MAIS
Restrictive fluid resuscitation in combination with damage control resuscitation: Time for adaptation.
Marquinn D et all. J Trauma Acute Care Surg. 2012;73: 674-678.
-------------------------------------------------------------------------------------------------------------
Ce travail confirme l'intérêt d'une stratégie de remplissage vasculaire parcimonieuse dès lors qu'une réanimation et une chirurgie spécialisée moderne sont accessibles. Le collectif des patients est ici celui de traumatisés thoraciques sévères arrivant dans une structure spécialisée dans des délais très courts. De telles conditions ne sont pas forcément celles de la prise en charge de blessés de guerre pour qui les délais d'évacuation sont souvent plus élevés. Il n'en demeure pas moins que cette publication milite pour une politique de remplissage vasculaire raisonnée. On rappelle que la procédure du sauvetage au combat donne pour objectif la perception d'un pouls radial perceptible.
-------------------------------------------------------------------------------------------------------------
BACKGROUND:
Damage control resuscitation (DCR) conveys a survival advantage in patients with severe hemorrhage. The role of restrictive fluid resuscitation (RFR) when used in combination with DCR has not been elucidated. We hypothesize that RFR, when used with DCR, conveys an overall survival benefit for patients with severe hemorrhage.
METHODS:
This is a retrospective analysis from January 2007 to May 2011 at a Level I trauma center. Inclusion criteria included penetrating torso injuries, systolic blood pressure less than or equal to 90 mm Hg, and managed with DCR and damage control surgery (DCS). There were two groups according to the quantity of fluid before DCS: (1) standard fluid resuscitation (SFR)greater than or equal to 150 mL of crystalloid; (2) RFR less than 150 mL of crystalloid. Demographics and outcomes were analyzed.
RESULTS:
Three hundred seven patients were included. Before DCS, 132 (43%) received less than 150 mL of crystalloids, grouped under RFR; and 175 (57%) received greater than or equal to 150 mL of crystalloids, grouped under SFR. Demographics and initial clinical characteristicswere similar between the study groups. Compared with the SFR group, RFR patients received less fluid preoperatively (129 mL vs. 2,757 mL; p G 0.001), exhibited a lower intraoperative mortality (9% vs. 32%; p G 0.001), and had a shorter hospital length of stay (13 vs. 18 days; p = 0.02). Patients in the SFR group had a lower trauma intensive care unit mortality (5 vs. 12%; p = 0.03) but exhibited a higher overall mortality. Patients receiving RFR demonstrated a survival benefit, with an odds ratio for mortality of 0.69 (95% confidence interval, 0.37Y0.91).

CONCLUSION:
To the best of our knowledge, this is the first civilian study that analyzes the impact of RFR in patients managed with DCR. Its use in conjunction with DCR for hypotensive trauma patients with penetrating injuries to the torso conveys an overall and early intraoperative survival benefit.
| Tags : remplissage, choc, hémorragie, perfusion
13/12/2011
25 recommandations UK pour les traumas jonctionnels
http://www.medicalsca.com/files/emf_parker_junctional_tra...
Une affaire d'équipe pour une prise en charge "aggressive" qu'il faut avoir réfléchi AVANT
| Tags : jonctionnel, hémorragie
08/12/2011
Document SFMU: Choc hémorragique en médecine de l'avant
| Tags : choc, hémorragie, remplissage, garrot, tourniquet
18/01/2011
Remplissage vasculaire et "Damage Control Resuscitation"
Pour compléter la note précédente, lisez la présentation proposée dans ce lien qui confirme le caractère relativement ténu des bases de certaines pratiques actuelles. Elle positionne le remplissage vasculaire comme un des éléments de la stratégie du "damage control resuscittaion", elle met en avant la prévention de l'hypothermie, elle rappelle les effets antiagrégants des hydroxy-ethylamidons et leur rôle néfastesur la formation du caillot de fibrine, ele rappelle l'intérêt de l'emploi d'antifibrinolytique comme l'acide tanexaminique (Exacyl) chez le traumatisé grave.
En ce qui concerne le sauvetage au combat:
la stratégie est
Perfuser en 20 min 250 ml de sérum salé hypertonique, suivi de 500 ml de macromolécules type VOLUVEN en cas non restauration de la perception du pouls radial et del'amélioration de la vigilence. Utiliser de l’adrénaline titrée IV (1 mg/10 ml ) en injectant ml par ml surtout si le blessé a été soumis à une explosion de forte puissance, dès la pose du second flacon de perfusion.
Réflechissez à
La prise en charge de l'hypothermie
L'emploi de l'exacyl qui est recommandé actuellement pour la prise en charge du polytraumatisé (Etude CRASH 2). Une autre étude confirme un intérêt encore plus important pour la prise en charge des blessés de guerre les plus hémorragiques(Etude Matters).
| Tags : remplissage, hémorragie
21/12/2010
Hydroxyethylamidon: Attention !
Cette revue de littérature rappelle quelques données essentielles sur l'emploi des HEA pour le remplissage vasculaire. Il en ressort que le bien fondé de cette pratique n'est pas validé y compris pour les HEA de 3ème génération 130/0,4 dont fait partie le voluven pourtant les moins sujets à complications. Ces dernières sont repréesntées par le risque d'insuffisance rénale, la tendance au saignement et une tendance à l'augmentation de la mortalité. Il n'est pas sans intérêt de faire remarquer que l'HYPERHES est un soluté contennat un HEA de type 2005.
Première lecture
REVIEW ARTICLE
The Efficacy and Safety of Colloid Resuscitation in the Critically Ill
Christiane S. Hartog, MD, Michael Bauer, MD, and Konrad Reinhart, MD
(Anesth Analg 2011;112:156 –64)
Despite evidence from clinical studies and meta-analyses that resuscitation with colloids or crystalloids is equally effective in critically ill patients, and despite reports from high-quality clinical trials and meta-analyses regarding nephrotoxic effects, increased risk of bleeding, and a trend toward higher mortality in these patients after the use of hydroxyethyl starch (HES) solutions, colloids remain popular and the use of HES solutions is increasing worldwide. We investigated the major rationales for colloid use, namely that colloids are more effective plasma expanders than crystalloids, that synthetic colloids are as safe as albumin, that HES solutions have the best risk/benefit profile among the synthetic colloids, and that the third-generation HES 130/0.4 has fewer adverse effects than older starches. Evidence from clinical studies shows that comparable resuscitation is achieved with considerably less crystalloid volumes than frequently suggested, namely, 2-fold the volume of colloids. Albumin is safe in intensive care unit patients except in patients with closed head injury. All synthetic colloids, namely, dextran, gelatin, and HES have dose-related side effects, which are coagulopathy, renal failure, and tissue storage. In patients with severe sepsis, higher doses of HES may be associated with excess mortality. The assumption that third-generation HES 130/0.4 has fewer adverse effects is yet unproven. Clinical trials on HES 130/0.4 have notable shortcomings. Mostly, they were not performed in intensive care unit or emergency department patients, had short observation periods of 24 to 48 hours, used cumulative doses below 1 daily dose limit (50 mL/kg), and used unsuitable control fluids such as other HES solutions or gelatins. In conclusion, the preferred use of colloidal solutions for resuscitation of patients with acute hypovolemia is based on rationales that are not supported by clinical evidence. Synthetic colloids are not superior in critically ill adults and children but must be considered harmful depending on the cumulative dose administered. Safe threshold doses need to be determine in studies in high-risk patients and observation periods of 90 days. Such studies on HES 130/0.4 are still lacking despite its widespread and increasing use. Because there are safer and
equally effective alternatives in the form of crystalloids, use of synthetic colloids should be avoided except in the context of clinical studies.
Seconde lecture
La Société Française d'anesthésie-réanimation rappelle d'ailleurs également ce risque hémorragique y compris pour les HEA 10/0,4 notamment lors d'adminsitration aiguë.
"
L’albumine, les gélatines et l’amidon 130 000/0,4 (Voluven®) n’interfèrent pas, ou quasiment pas avec l’hémostase. La prudence reste toutefois conseillée : Comentaires Ainsi les effets secondaires des HEA ne sont pas que liés à eur adminsitration répétitive. Dans nos conditions d'emploi , il apparait nécessaire d'observer une certaine retenue dans ll'usage des HEA. Ceci plaide pour l'utilisation des solutés cristalloïdes tel que le Ringer lactate, le sérum salé hypertonique et pose la question d'un recours plus large au gélatines fluides modifiées malgré leur risque allergique (?)
- chez les patients insuffisants rénaux
- en cas de perfusion prolongée ou de volume de colloïdes important ;
- en cas de troubles de l’hémostase acquis ;
- chez les patients traités par antiplaquettaires ou anticoagulants ;
- en présence d’une anémie ou thrombopénie profonde ;
- chez les patients porteurs d’une maladie de Willebrand ;
- chez les patients de groupe sanguin O (ces patients ont spontanément un taux de Willebrand plus bas) ;
- en présence d’un saignement chirurgical actif ;
- en présence d’une transfusion massive ou d’une hypothermie.
| Tags : remplissage, choc, hémorragie
30/11/2010
Contrôler une hémorragie
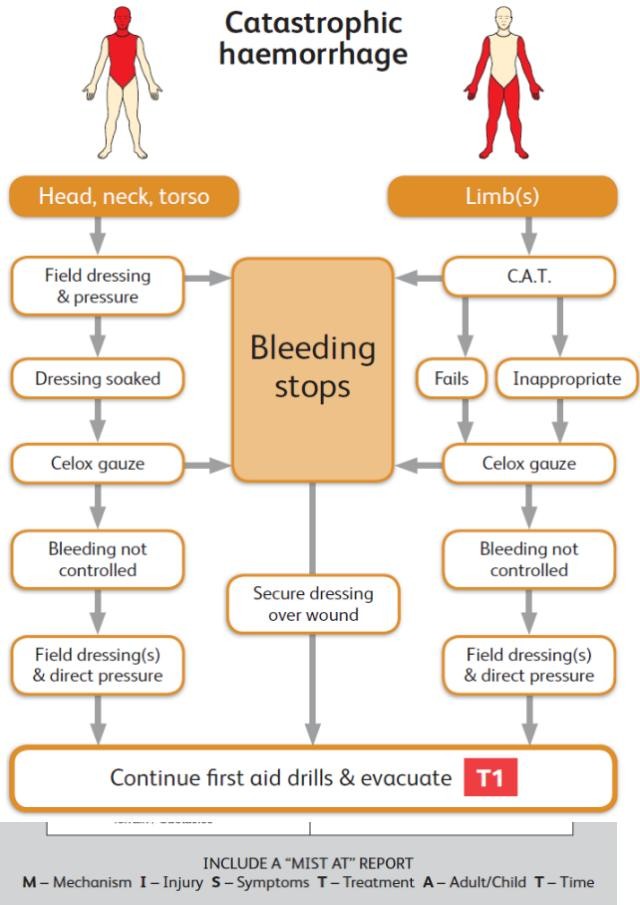
| Tags : hémorragie, tourniquet, garrot