11/01/2015
Histoire de casque de protection
Ballistic helmets – Their design, materials, and performance against traumatic brain injury
Kulkarni SG et Al. Composite Structures 101 (2013) 313–331
Protecting a soldier’s head from injury is critical to function and survivability. Traditionally, combat helmets have been utilized to provide protection against shrapnel and ballistic threats, which have reduced head injuries and fatalities. However, home-made bombs or improvised explosive devices (IEDs) have been increasingly used in theatre of operations since the Iraq and Afghanistan conflicts. Traumatic brain injury (TBI), particularly blast-induced TBI, which is typically not accompanied by external body injuries, is becoming prevalent among injured soldiers. The responses of personal protective equipment, especially combat helmets, to blast events are relatively unknown. There is an urgent need to develop head protection systems with blast protection/mitigation capabilities in addition to ballistic protection.
Modern military operations, ammunitions, and technology driven war tactics require a lightweight headgear that integrates protection mechanisms (against ballistics, blasts, heat, and noise), sensors, night vision devices, and laser range finders into a single system.
The current article provides a comparative study on the design, materials, and ballistic and blast performance of the combat helmets used by the US Army based on a comprehensive and critical review of existing studies. Mechanisms of ballistic energy absorption, effects of helmet curvatures on ballistic performance, and performance measures of helmets are discussed. Properties of current helmet materials (including Kevlar K29, K129 fibers and thermoset resins) and future candidate materials for helmets (such as nano-composites and thermoplastic polymers) are elaborated. Also, available experimental and computational studies on blast-induced TBI are examined, and constitutive models developed for brain tissues are reviewed. Finally, the effectiveness of current combat helmets against TBI is analyzed along with possible avenues for future research.
| Tags : balistique, blast, tbi
15/10/2013
Dehors et dedans, ce n'est pas la même chose
Primary blast lung injury prevalence and fatal injuries from explosions: Insights from postmortem computed tomographic analysis of 121 improvised explosive device fatalities
SIngleton JAG et all. J Trauma Acute Care Surg. 2013;75: S269-S274.
BACKGROUND:
Primary blast lung injury (PBLI) is an acknowledged cause of death in explosive blast casualties. In contrast to vehicle occupants following an in-vehicle explosion, the injury profile, including PBLI incidence, for mounted personnel following an external explosion has yet to be as well defined.
METHODS:
This retrospective study identified 146 cases of UK military personnel killed by improvised explosive devices (IEDs) between November 2007 and July 2010. With the permission of Her Majesty's Coroners, relevant postmortem computed tomography imaging was analyzed. PBLI was diagnosed by postmortem computed tomography. Injury, demographic, and relevant incident data were collected via the UK Joint Theatre Trauma Registry.
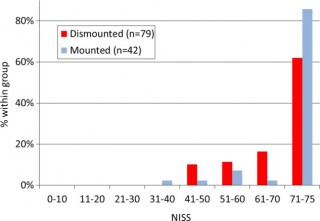
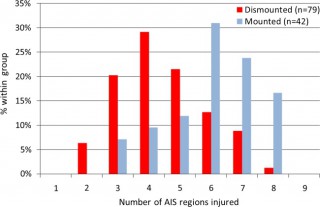
RESULTS:
Autopsy results were not available for 1 of 146 cases. Of the remaining 145 IED fatalities, 24 had catastrophic injuries (disruptions), making further study impossible, leaving 121 cases; 79 were dismounted (DM), and 42 were mounted (M). PBLI was noted in 58 cases, 33 (79%) of 42 M fatalities and 25 (32%) of 79 DM fatalities (p < 0.0001). Rates of associated thoracic trauma were also significantly greater in the M group (p < 0.006 for all). Fatal head (53% vs. 23%) and thoracic trauma (23% vs. 8%) were both more common in the M group, while fatal lower extremity trauma (7% vs. 48%) was more commonly seen in DM casualties (p < 0.0001 for all).
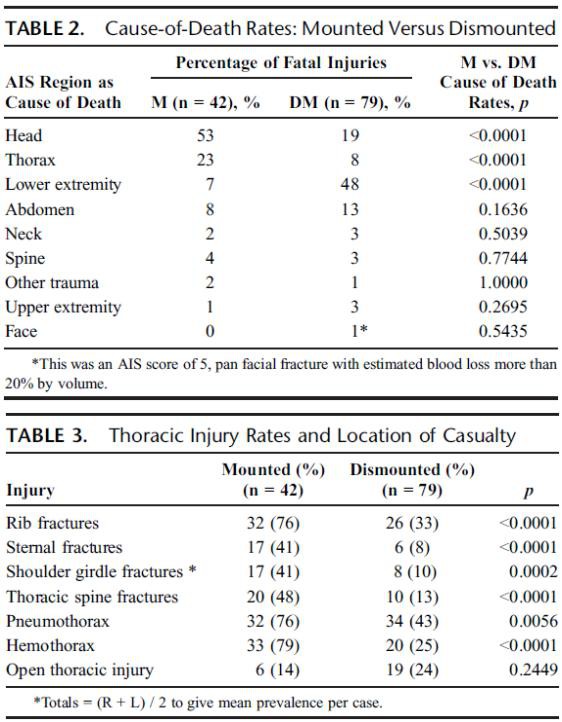
CONCLUSION:
Following IED strikes, mounted fatalities are primarily caused by head and chest injuries. Lower extremity trauma is the leading cause of death in dismounted fatalities. Mounted fatalities have a high incidence of PBLI, suggesting significant exposure to primary blast. This has not been reported previously. Further work is required to determine the incidence and clinical significance of this severe lung injury in explosive blast survivors. In addition, specific characteristics of the vehicles should be considered.
| Tags : blast, balistique
21/09/2013
Contamination des plaies: A l'entrée et la sortie
Effect of Initial Projectile Speed on Contamination Distribution in a Lower Extremity Surrogate “Wound Track”
Krebsbach MA et All., Military Medicine, 177, 5:573, 2012
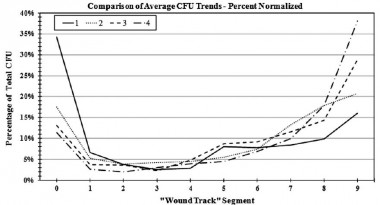
Le nettoyage précoce et la couverture des orifices d'entrée et de sortie sont donc théoriquement des maillons importants de la lutte contre l'infection des plaies de guerre.
| Tags : infection, balistique, pansement
07/09/2013
Causes de DC évitables: Actualisation UK
Identifying future ‘unexpected’ survivors: a retrospective cohort study of fatal injury patterns in victims of improvised explosive devices
To identify potentially fatal injury patterns in explosive blast fatalities in order to focus research and mitigation strategies, to further improve survival rates from blast trauma.
DESIGN:
Retrospective cohort study.
PARTICIPANTS:
UK military personnel killed by improvised explosive device (IED) blasts in Afghanistan, November 2007-August 2010.
SETTING:
UK military deployment, through NATO, in support of the International Security Assistance Force (ISAF) mission in Afghanistan.
DATA SOURCES:
UK military postmortem CT records, UK Joint Theatre Trauma Registry and associated incident data.
MAIN OUTCOME MEASURES:
Potentially fatal injuries attributable to IEDs.
RESULTS:
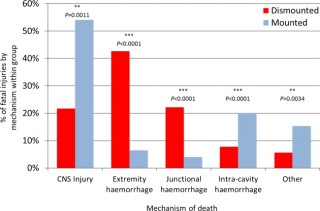
We identified 121 cases, 42 mounted (in-vehicle) and 79 dismounted (on foot), at a point of wounding. There were 354 potentially fatalinjuries in total. Leading causes of death were traumatic brain injury (50%, 62/124 fatal injuries), followed by intracavity haemorrhage (20.2%, 25/124) in the mounted group, and extremity haemorrhage (42.6%, 98/230 fatal injuries), junctional haemorrhage (22.2%, 51/230 fatal injuries) and traumatic brain injury (18.7%, 43/230 fatal injuries) in the dismounted group.
CONCLUSIONS:
Head trauma severity in both mounted and dismounted IED fatalities indicated prevention and mitigation as the most effective strategies to decrease resultant mortality. Two-thirds of dismounted fatalities had haemorrhage implicated as a cause of death that may have been anatomically amenable to prehospital intervention. One-fifth of the mounted fatalities had haemorrhagic trauma which currently could only be addressed surgically. Maintaining the drive to improve all haemostatic techniques for blast casualties, from point of wounding to definitive surgical proximal vascular control, alongside the development and application of novel haemostatic interventions could yield a significant survival benefit. Prospective studies in this field are indicated.
Cette publication est très importante car elle insiste sur l'absolue nécessité de poursuivre les efforts en vue de prévenir le trauma aussi bien en matière de protection balistique, de réduction des délais de transports pour permettre la prise en charge d'hémorragie intra-cavitaires et l'aspect fondamental d'arrêter toutes les hémorragies sur le terrain notamment pas la mise en oeuvre d'une nouvelle catégorie de garrots pour les hémorragies jonctionnelles (voir 1, 2, 3, 4, 5, 6)
Les morts par IED sont plus sévèrement atteints dans un véhicule qu'à pied.
58% des Décès sont liés à plus de 2 causes potentiellement évitables
Les causes de décès ne sont pas les mêmes en combat à pied ou en véhicule
| Tags : balistique, blast, traumatologie, explosion, jonctionnel
25/06/2013
Blast TBI: Un seuil plus bas que pour le poumon
Working toward exposure thresholds for blast-induced traumatic brain injury: thoracic and acceleration mechanisms.
Courtney MW et all. Neuroimage, 2011 Jan,54 Suppl 1: S55-61
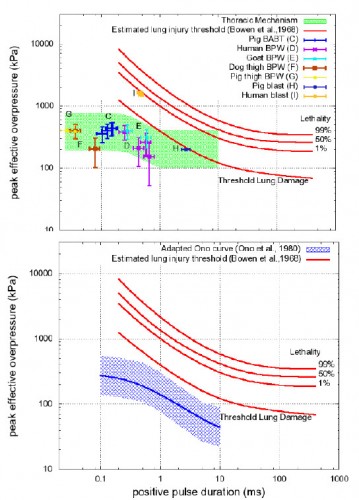
Les mécanismes du blast cérébral associent la tansmission de la surpression via le thorax, l'impact direct sur la boite crânienne et les phénomènes d'accélaration de l'extrémité céphalique. Ce document explore la première voie et exprime bien que les seuils lésionnels de lésions cérébrales (courbes de Ono) sont plus bas que les seuils pulmonaires(courbes de Bowden).
| Tags : balistique, tbi
23/05/2013
Ballistic trauma. A practical guide
| Tags : balistique
26/03/2013
Mesurer l'exposition au blast: Une réalité
La nécessité de connaître le niveau d'exposition à une onde de blast commence à devenir évidente.Des dispositifs adaptés appraissent sur le marché. Parmi ceux ci le BLAST GAUGE semble intéressant. Porté sur le casque, le gilet pare-balle ou tout autre surface il enregistre l'onde de pression, permet la reconnaissance du niveau par led colorée et l'analyse de la courbe par récupération des données sur un ordinateur.
Le dispositif
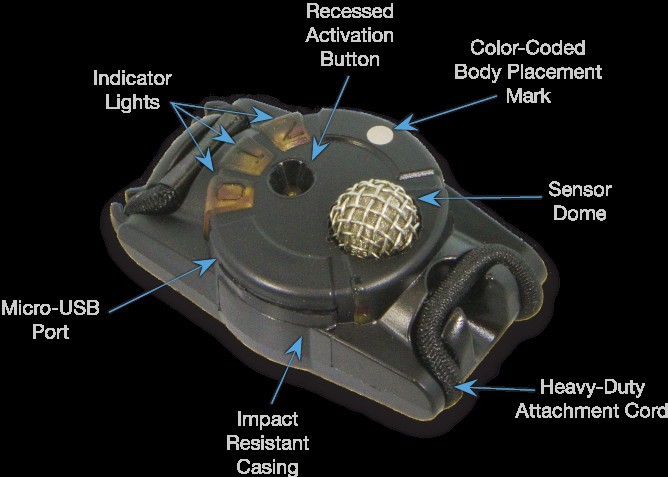
Port sur le casque

D'autres systèmes sont proposés comme le système HEADS de la société BAE dont près de 20 000 dispositfs ont été fournis à l'amée américaine et il est hautement propable que ce type de ce produit va très rapidement être mis en oeuvre dès lors qu'une expsoition à de fortes explosions notamment en milieu clos est attendue.
| Tags : blast, balistique
21/03/2013
Immobilisation du rachis: Dès que possible ! Surtout si VBIED
J Trauma Acute Care Surg. 2013;74: 1112-1118
Si l'atteinte du rachis cervical était dans les derniers conflits est de l'ordre de 1 à 2%, ce taux est monté à 5-8% dans le conflit irakien. Ceci s'explique par l'émergence d'un nouveau mécanisme d'aggression par IED. La procédure du sauvetage au combat stipule que l'imobilisation du rachis cervical ne doit pas être réalisée sous le feu direct de l'ennemi. La frequence des lésions du rachis dans les combats actuels l'impose cependant dès que blessé et sauveteurs sont à l'abri surtout si il s'agit d'un VBIED. C'est que suggère cette publication édifiante qui porte sur l'analyse des lésions du rachis cervical chez les soldats décédés.
| Tags : rachis, balistique
17/02/2013
Ballistic trauma. A practical guide
| Tags : balistique
26/01/2013
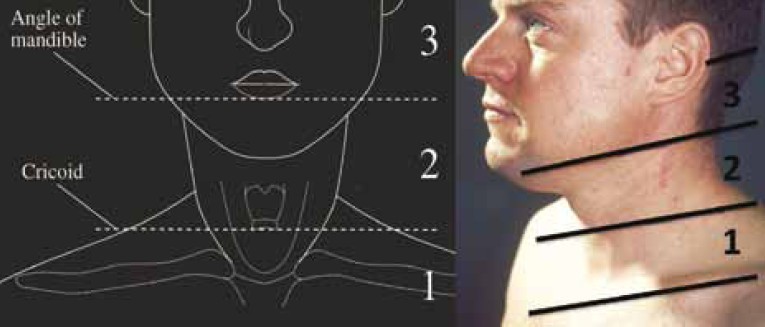
Lésions du cou: Le point UK
Outcomes from Penetrating Ballistic Cervical Injury
Breeze J et all.J R Army Med Corps 158(2): 96-100
Aims:
Ballistic cervical injury has become a significant source of both morbidity and mortality for the deployed UK soldier. The aim of this paper was to document a case series of ballistic cervical wounds to describe the pattern of these injuries and relate them to outcome.
Methods:
The records of all UK service personnel sustaining wounds to the neck in Iraq or Afghanistan between 01 August 2004 and 01 January 2008 were analysed following identification by the Joint Theatre Trauma Registry. Blunt or thermal injuries were excluded.
Results:
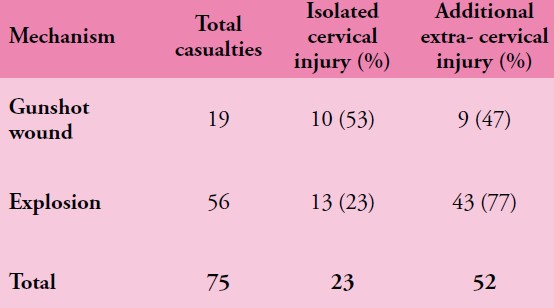
The records of 75/76 service personnel sustaining penetrating cervical injury during this period were available for analysis. 56/75 (75%) were due to explosive fragmentation and the remainder due to gunshot wounds (GSW). 33/75 (44%) of soldiers sustained vascular injury, 32/75 (43%) injury to the spine or spinal cord, 29/75 (39%) injury to the larynx or trachea and 11/75 (15%) injury to the pharynx or oesophagus. 14/75 (19%) patients in this series underwent surgery in a hospital facility for treatment of potentially life threatening cervical injuries, with a survival rate after surgery of 12/14 (86%). The overall mortality from this series of battlefield penetrating neck injury was 63%.

Conclusions:
Penetrating cervical ballistic injury is a significant source of injury to deployed UK service personnel, predominantly due to neurovascular damage. Neck collars if worn would likely prevent many of the injuries in this case series but such protection is uncomfortable and may interfere with common military tasks. Newer methods of protecting the neck should be investigated that will be acceptable to the deployed UK soldier.
| Tags : maxillo, cou, balistique
06/07/2012
Balistique: Actualisation OEF/OIF
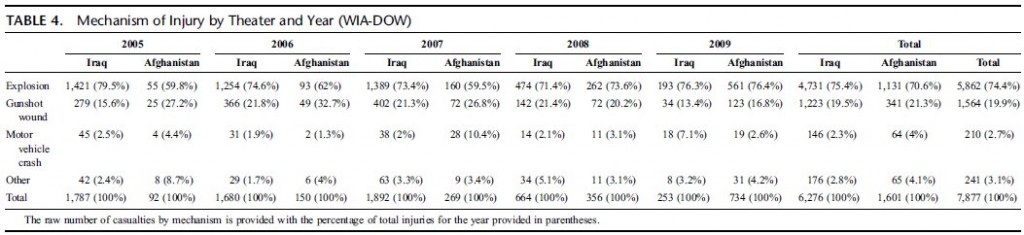
Combat wounds in Iraq and Afghanistan from 2005 to 2009
J Belmont JP et all. (J Trauma Acute Care Surg. 2012;73: 3-12)
Morceaux choisis:
Among the 1,992,232 military service members who were deployed, there were 29,624 distinct combat wounds in 7,877 combat casualties. The mean age of the combat casualty cohort was 26.0 years old. The combat casualties were predominantly male (98I8%), Army (77,5%), and junior enlisted (59,0%). The distribution of combat wounds was as follows: head/neck, 28,1%; thorax, 9,9%; abdomen, 10,1%; and extremities, 51,9%. Explosive injury mechanisms accounted for 74,4% of all combat casualties, which was significantly higher than those caused by gunshot wounds (19,9%) (p G 0.0001). From 2005 to 2007, explosive mechanisms of injury were significantly more common in Iraq than in Afghanistan (p G 0.001). The percentage of explosive mechanisms increased significantly in Afghanistan between the years 2007 (59,5%) and 2008 (73,6%) ( p < 0.0003)
In addition, 1,064 (13,5%) of all combat casualties also sustained burn injuries
| Tags : balistique
03/06/2012
VBIED: Le point UK
In-vehicle extremity injuries from improvised explosive devices: current and future foci
Ramasamy A et all. Phil. Trans. R. Soc. B 2011 366, 160-170
The conflicts in Iraq and Afghanistan have been epitomized by the insurgents’ use of the improvised explosive device against vehicle-borne security forces. These weapons, capable of causing multiple severely injured casualties in a single incident, pose the most prevalent single threat to Coalition troops operating in the region. Improvements in personal protection and medical care have resulted in increasing numbers of casualties surviving with complex lower limb injuries, often leading to long-term disability. Thus, there exists an urgent requirement to investigate and mitigate against the mechanism of extremity injury caused by these devices. This will necessitate an ontological approach, linking molecular, cellular and tissue interaction to physiological dysfunction. This can only be achieved via a collaborative approach between clinicians, natural scientists and engineers, combining physical and numerical modelling tools with clinical data from the battlefield. In this article, we compile existing knowledge on the effects of explosions on skeletal injury, review and critique relevant experimental and computational research related to lower limb injury and damage and propose research foci required to drive the development of future mitigation technologies.

| Tags : balistique
01/01/2011
Balistique terminale: Historique

| Tags : balistique