21/07/2018
AP-IED: +grave que mine
Injury profile suffered by targets of antipersonnel improvised explosive devices: prospective cohort study
Victims of AP-IED were more likely, compared with APM victims, to have multiple amputations (70.0% vs 10.4%; p<0.001) or genital injury (26% vs 13%; p=0.007). Multiple amputations occurred in 70 patients: 5 quadruple amputations, 27 triple amputations and 38 double amputations. Pelvic fracture occurred in 21 victims, all but one of whom had multiple amputations. Severe perineal, gluteal or genital injuries were present in 46 patients. Severe soft tissue injury was universal, with injection of contaminated soil along tissue planes well above entry sites. There were 13 facial injuries, 9 skull fractures and 3 traumatic brain injuries. Eleven eye injuries were seen; none of the victims with eye injuries were wearing eye protection. The casualty fatality rate was at least 19%. The presence of more than one amputation was associated with a higher rate of pelvic fracture (28.6% vs 3.3%; p=0.005) and perineal–gluteal injury (32.6% vs 11.1%; p=0.009).
The injury pattern suffered by the target of the AP-IED is markedly worse than that of conventional APM. Pelvic binders and tourniquets should be applied at the point of injury to patients with multiple amputations or perineal injuries.
| Tags : blast
30/06/2017
Trauma sonore: Protection et corticoïdes
Acute Acoustic Trauma among Soldiers during an Intense Combat.
-----------------------------------
BACKGROUND:
During military actions, soldiers are constantly exposed to various forms of potentially harmful noises. Acute acoustic trauma (AAT) results from an impact, unexpected intense noise ≥140 dB, which generates a high-energy sound wave that can damage the auditory system.
PURPOSE:
We sought to characterize AAT injuries among military personnel during operation "Protective Edge," to analyze the effectiveness of hearing protection devices (HPDs), and to evaluate the benefit of steroid treatment in early-diagnosed AAT injury.
RESEARCH DESIGN:
We retrospectively identified affected individuals who presented to military medical facilities with solitary or combined AAT injuries within 4 mo following an intense military operation, which was characterized with an abrupt, intensive noise exposure (July-December 2014).
STUDY SAMPLE:
A total of 186 participants who were referred during and shortly after a military operation with suspected AAT injury.
INTERVENTIONS:
HPDs, oral steroids.
DATA COLLECTION AND ANALYSIS:
Data extracted from charts and audiograms included demographics, AAT severity, worn HPDs, first and last audiograms and treatment (if given). The Student's independent samples t test was used to compare continuous variables. All tests were considered significant if p values were ≤0.05.
RESULTS:
A total of 186 participants presented with hearing complaints attributed to AAT: 122, 39, and 25 were in duty service, career personnel, and reservists, with a mean age of 21.1, 29.2, and 30.4 yr, respectively. Of them, 92 (49%) participants had confirmed hearing loss in at least one ear. Hearing impairment was significantly more common in unprotected participants, when compared with protected participants: 62% (74/119) versus 45% (30/67), p < 0.05. Tinnitus was more common in unprotected participants when compared with protected participants (75% versus 49%, p = 0.04), whereas vertigo was an uncommon symptom (5% versus 2.5%, respectively, p > 0.05). In the 21 participants who received steroid treatment for early-diagnosed AAT, bone-conduction hearing thresholds significantly improved in the posttreatment audiograms, when compared with untreated participants (p < 0.01, for 1-4 kHz).
CONCLUSIONS:
AAT is a common military injury, and should be diagnosed early to minimize associated morbidity. HPDs were proven to be effective in preventing and minimizing AAT hearing sequelae. Steroid treatment was effective in AAT injury, if initiated within 7 days after noise exposure.
| Tags : blast
09/10/2016
Blessés des combats modernes:Spécifiques
A modern combat trauma
INTRODUCTION:
The world remains plagued by wars and terrorist attacks, and improvised explosive devices (IED) are the main weapons of our current enemies, causing almost two-thirds of all combat injuries. We wished to analyse the pattern of blast trauma on the modern battlefield and to compare it with combat gunshot injuries.
MATERIALS AND METHODS:
Analysis of a consecutive series of combat trauma patients presenting to two Bulgarian combat surgical teams in Afghanistan over 11 months. Demographics, injury patterns and Injury Severity Scores (ISS) were compared between blast and gunshot-injured casualties using Fisher's Exact Test.
RESULTS:
The blast victims had significantly higher median ISS (20.54 vs 9.23) and higher proportion of ISS>16 (60% vs 33.92%, p=0.008) than gunshot cases. They also had more frequent involvement of three or more body regions (47.22% vs 3.58%, p<0.0001). A significantly higher frequency of head (27.27% vs 3.57%), facial (20% vs 0%) and extremities injuries (85.45% vs 42.86%) and burns (12.72% vs 0%) was noted among the victims of explosion (p<0.0001). Based on clinical examination and diagnostic imaging, primary blast injury was identified in 24/55 (43.6%), secondary blast injury in 37 blast cases (67.3%), tertiary in 15 (27.3%) and quaternary blast injury (all burns) in seven (12.72%).
CONCLUSIONS:
Our results corroborate the 'multidimensional' injury pattern of blast trauma. The complexity of the blast trauma demands a good knowledge and a special training of the military surgeons and hospital personnel before deployment.
| Tags : blast
12/01/2016
Dexamethasone: Hémostatique cérébral ?
Steroid-loaded Hemostatic Nanoparticles Alleviate Injury Progression after Blast Trauma
Hubbard WD et Al.. ACS Macro Lett., 2015, 4 (4), pp 387–391
The purpose of this study was to investigate whether hemostatic dexamethasone-loaded nanoparticles (hDNP) functionalized with a peptide that binds with activated platelets could reduce cellular injury and improve functional outcomes in a model of blast trauma. Functionalized nanoparticles, or synthetic platelets, offer a wide variety of benefits and advantages compared to alternatives, such as increased biocompatibility and targeting of the injury site (DePalma, 2005). Blood loss is the primary cause of death at acute time points post injury in both civilian and battlefield traumas. Currently, there is a shortage in treatments for internal bleeding, especially for rapid administration in open field combat. In a recent U.K. study, less than fifty percent of soldiers diagnosed with primary blast lung injury (PBLI), the most common fatal blast injury, survived to reach a medical facility (Smith, 2011). This study examines potential therapeutic effects of hDNP on subacute recovery in brain pathology and behavior after blast polytrauma. An established polytrauma model that simulates severe injury, including PBLI and blast-induced neurotrauma (BINT), can be used to evaluate life-saving therapeutics (Hubbard, 2014). Poly(lactic-co-glycolic acid)-based nanoparticles with poly(ethylene glycol) arms and the arginine-glycine-aspartic acid (RGD) peptide to target activated platelets were fabricated. A blast-induced polytrauma rodent model was used to evaluate the functionalized nanoparticles at an acute stage. After anesthesia, Male Sprague Dawley rats were exposed to a single, representative “free field” blast wave from an Advanced Blast Simulator at Virginia Tech at a peak overpressure of 28 psi for 2.5 ms duration, operating above 50% lethality risk, in a sidethorax orientation (Hubbard, 2014). After injury, animals were immediately injected intravenously with hDNP, control dexamethasone-loaded nanoparticles (cDNP), or lactated ringers (LR) and physiological parameters were monitored. Sham animals were not injected or exposed to the blast wave. Open field assays were performed on surviving animals to measure levels of anxiety. At one week post-blast, brains were extracted and sections from the amygdala were obtained for immunofluorescent staining using glial fibrillary acidic protein (GFAP; activated astrocytes), cleaved caspase-3 (apoptosis), and SMI-71 (blood-brain barrier). According to physiological monitoring immediately after blast, oxygen saturation was significantly decreased in the control and LR groups compared to the active and sham groups. Using the open field test, elevated anxiety parameters were found in the control and LR groups compared to the hDNP group. GFAP was significantly elevated in the control group compared to the hDNP and sham groups in the amygdala. Caspase-3 was also significantly elevated in the control group compared to the hDNP group. SMI-71 was significantly reduced in the LR group compared to the sham group. hDNP treatment has the potential to assist recovery after internal hemorrhage. Immediate intervention to assuage hemorrhage, one source for injury pathology, is crucial to mitigate debilitating injury mechanisms that lead to cognitive and emotional deficits (Shetty, 2014).

It is possible that through prevention of microhemorrhaging of the blood-brain barrier (BBB), hDNP was able to mitigate cellular injury and improve cognitive outcomes. Future studies will evaluate the effect on inflammatory and hypoxia-related proteins after hDNP administration post-trauma.
| Tags : blast, hémorragie
19/12/2015
Amputé des jambes: Le bassin aussi !
The incidence of pelvic fractures with traumatic lower limb amputation in modern warfare due to improvised explosive devices
Cross AM et Al. J R Nav Med Serv 2014;100(2):152-6
---------------------------------------------
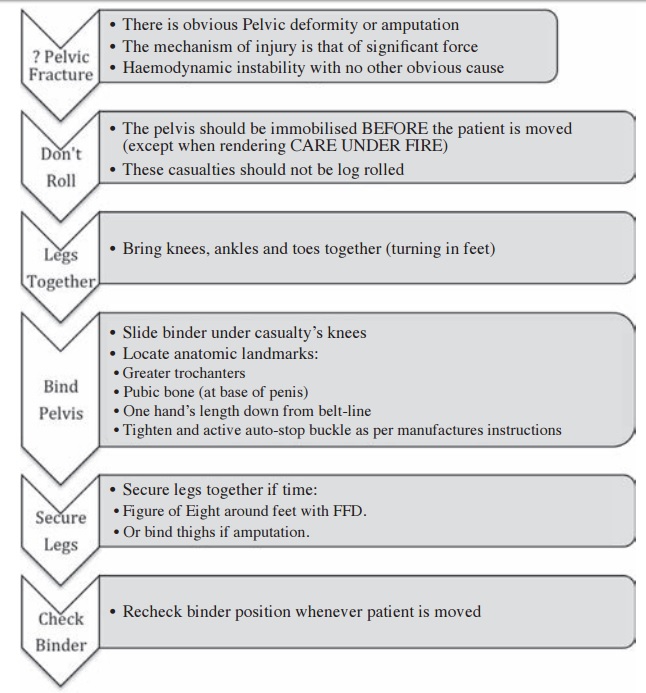
Excepté l'extraction d'urgence de blessés sous le feu, la prise en charge den cas d'amputation traumatique doit inclure la forte probabilité de traumatisme du bassin. Une utilisation large des immobilisations pelviennes doit donc être à l'esprit. On rappelle simplement la gravité et la difficulté de prise en charge des hémorragies liées aux fractures de bassin.
---------------------------------------------
AIMS:
A frequently-seen injury pattern in current military experience is traumatic lower limb amputation as a result of improvised explosive devices (IEDs). This injury can coexist with fractures involving the pelvic ring. This study aims to assess the frequency of concomitant pelvic fracture in IED-related lower limb amputation.
METHODS:
A retrospective analysis of the trauma charts, medical notes, and digital imaging was undertaken for all patients arriving at the Emergency Department at the UK military field hospital in Camp Bastion, Afghanistan, with a traumatic lower limb amputation in the six months between September 2009 and April 2010, in order to determine the incidence of associated pelvic ring fractures.
RESULTS:
Of 77 consecutive patients with traumatic lower limb amputations, 17 (22%) had an associated pelvic fracture (eleven with displaced pelvic ring fractures, five undisplaced fractures and one acetabular fracture). Unilateral amputees (n = 31) had a 10% incidence of associated pelvic fracture, whilst 30 % of bilateral amputees (n = 46) had a concurrent pelvic fracture. However, in bilateral, trans-femoral amputations (n = 28) the incidence of pelvic fracture was 39%.
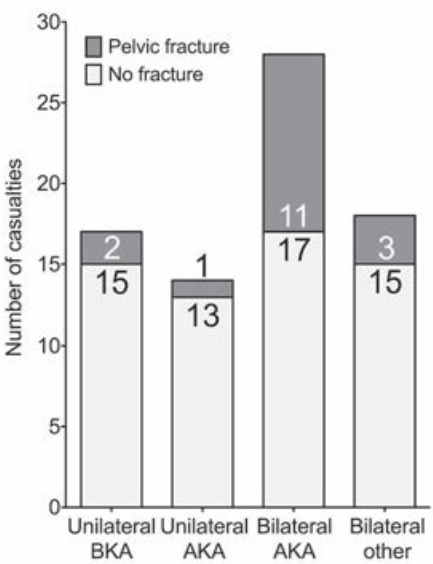
CONCLUSIONS:
The study demonstrates a high incidence of pelvic fractures in patients with traumatic lower limb amputations, supporting the routine pre-hospital application of pelvic binders in this patient group
| Tags : hémorragie, immobilisation, blast
28/03/2015
Blast et squelette osseux: Lésions spécifiques ?
Blast Injury and the Human Skeleton: An Important Emerging Aspect of Conflict-Related Trauma.
Dussault C. et Al. J Forensic Sci. 2014 May;59(3):606-12 [Thèse]
--------------------------------------------------------------------
La rupture de la membrane du tympan en cas serait un marqueur peu fiable du blast et de sa gravité (1,2, 3). Il semblerait que certaines lésions osseuses soient assez spécifiques de blast osseux. Ceci a son intérêt en médecine médico-légale quand les circonstances de décès ne sont pas connues.
--------------------------------------------------------------------
Recent decades have seen an accelerating trend in warfare whereby a growing proportion of conflict-related deaths have been caused by explosions. Analysis of blast injury features little in anthropological literature. We present a review of clinical literature that includes prevalence of injury to anatomical regions and potential indicators of blast injury which can be used by forensic anthropologists. This includes high prevalence of extremity (22.8–91.2%) and facial (19.6–40%) injury in combat contexts, lower limb fractures (19–74.3%) in suicide bombing, traumatic amputation (3–43%) and diffuse fracture patterns in terrorist bombings. Potential indicators of blast trauma include blowout fractures in sinus cavities from blast overpressure, transverse mandibular fractures, and visceral surface rib fractures. Ability to recognize blast trauma and distinguish it in the skeleton is of importance in investigations and judicial proceedings relating to war crimes, terrorism, and human rights violations and likely to become increasingly crucial to forensic anthropology knowledge.
--------------------------------------------------------------------
1. Les factures mandibulaires transverses
[Mandibular fractures in British military personnel secondary to blast trauma sustained in Iraq and Afghanistan. Breeze et al. Br J Oral Maxillofac Surg. 2011 Dec;49(8):607-11]
Elles portent essentiellement sur la symphyse et le corps alors qu'en traumatologie civile il s'agit essentiellement d'atteintes du condyle et de l'angle
2. Les fractures de plancher de type "Blow out"
Le cadre orbitaire reste intact. Le plancher de l'orbite est atteint. Il y a irruption du contenu orbitaire dans le sinus. Le risque est que ces fractures passent inaperçues. Cliniquement elle se traduise par une anomalie de l'occulomotricité.
3. Les fractures de cotes en aile de papillon
[Rib Butterfly Fractures as a Possible Indicator of Blast Trauma. Christensen et Al. J Forensic Sci. 2013 Jan;58 Suppl 1:S15-9.]

| Tags : blast
11/01/2015
Histoire de casque de protection
Ballistic helmets – Their design, materials, and performance against traumatic brain injury
Kulkarni SG et Al. Composite Structures 101 (2013) 313–331
Protecting a soldier’s head from injury is critical to function and survivability. Traditionally, combat helmets have been utilized to provide protection against shrapnel and ballistic threats, which have reduced head injuries and fatalities. However, home-made bombs or improvised explosive devices (IEDs) have been increasingly used in theatre of operations since the Iraq and Afghanistan conflicts. Traumatic brain injury (TBI), particularly blast-induced TBI, which is typically not accompanied by external body injuries, is becoming prevalent among injured soldiers. The responses of personal protective equipment, especially combat helmets, to blast events are relatively unknown. There is an urgent need to develop head protection systems with blast protection/mitigation capabilities in addition to ballistic protection.
Modern military operations, ammunitions, and technology driven war tactics require a lightweight headgear that integrates protection mechanisms (against ballistics, blasts, heat, and noise), sensors, night vision devices, and laser range finders into a single system.
The current article provides a comparative study on the design, materials, and ballistic and blast performance of the combat helmets used by the US Army based on a comprehensive and critical review of existing studies. Mechanisms of ballistic energy absorption, effects of helmet curvatures on ballistic performance, and performance measures of helmets are discussed. Properties of current helmet materials (including Kevlar K29, K129 fibers and thermoset resins) and future candidate materials for helmets (such as nano-composites and thermoplastic polymers) are elaborated. Also, available experimental and computational studies on blast-induced TBI are examined, and constitutive models developed for brain tissues are reviewed. Finally, the effectiveness of current combat helmets against TBI is analyzed along with possible avenues for future research.
| Tags : balistique, blast, tbi
20/12/2014
La NAC: Intéressante en role 1: Probable ?
La N-acétylcystéine ou acétylcystéine ou NAC est un acide aminé non essentiel, qui stimule la production de glutathion, un antioxydant. Elle est surtout connue comme agent mucolytique. En médecine d'urgence son emploi lors d'intoxication au paracétamol est parfaitement validé. Moins connues sont les emplois de cet agent antioxydant dans deux types d'indication qui nous intéressent.
La première est le traumatisme sonore aigu notamment après explosion (1) ou tir (2) où il semblerait que la démarche classique [repos auditif, corticothérapie+/- vasodilatateurs] (3, 4) évoluerait vers une statégie associant le repos, la corticothérapie et unhe stratégie antioxydante précoce incluant le recours précoce à la N Acétyl Cystéine(5, 6).
La seconde porte sur la réduction des séquelles neurologiques après blast cérébral (7). Cet intérêt pour les effets anti-oxydants ne sont pas nouveaux et les effets «protecteurs» sont mis en avant également au niveau pulmonaire (8), rénale (9) et hépatique (10).
Si tout ceci reste à valider (11, 12), il semble que l'intégration de cette molécule ancienne soit d'un intérêt réel pour la prise en charge du combattant blasté ou exposéà un TSA à condition que l'administration soit précoce (<1h) (13) et donc que la N Acétyl Cystéine soit disponible en rôle 1
16/11/2013
NAC après une explosion: Bon pour le neurone.
Amelioration of Acute Sequelae of Blast Induced Mild Traumatic Brain Injury by N-Acetyl Cysteine: A Double- Blind, Placebo Controlled Study
Hoffer ME et Al. PLoS One. 2013;8(1):e54163. doi: 10.1371/journal.pone.0054163. Epub 2013 Jan 23.
Background: Mild traumatic brain injury (mTBI) secondary to blast exposure is the most common battlefield injury in Southwest Asia. There has been little prospective work in the combat setting to test the efficacy of new countermeasures. The goal of this study was to compare the efficacy of N-acetyl cysteine (NAC) versus placebo on the symptoms associated with blast exposure mTBI in a combat setting.
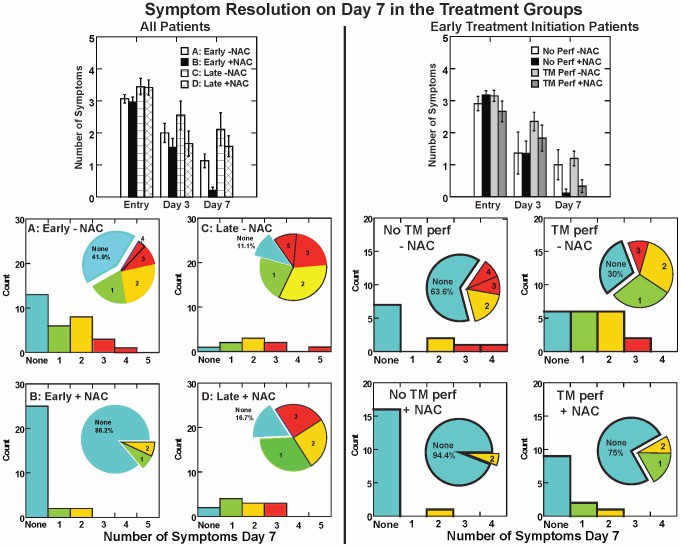
Methods: This study was a randomized double blind, placebo-controlled study that was conducted on active duty service members at a forward deployed field hospital in Iraq. All symptomatic U.S. service members who were exposed to significant ordnance blast and who met the criteria for mTBI were offered participation in the study and 81 individuals agreed to participate. Individuals underwent a baseline evaluation and then were randomly assigned to receive either N- acetyl cysteine (NAC) or placebo for seven days.
4 g per os puis 18-24h après 2X2 g jusqu'à J4 puis 1,5 g X2 jusqu'à J7
Each subject was re-evaluated at 3 and 7 days. Outcome measures were the presence of the following sequelae of mTBI: dizziness, hearing loss, headache, memory loss, sleep disturbances, and neurocognitive dysfunction. The resolution of these symptoms seven days after the blast exposure was the main outcome measure in this study. Logistic regression on the outcome of ‘no day 7 symptoms’ indicated that NAC treatment was significantly better than placebo (OR = 3.6, p = 0.006). Secondary analysis revealed subjects receiving NAC within 24 hours of blast had an 86% chance of symptom resolution with no reported side effects versus 42% for those seen early who received placebo.
Conclusion: This study, conducted in an active theatre of war, demonstrates that NAC, a safe pharmaceutical countermeasure, has beneficial effects on the severity and resolution of sequelae of blast induced mTBI. This is the first demonstration of an effective short term countermeasure for mTBI. Further work on long term outcomes and the potential use of NAC in civilian mTBI is warranted
| Tags : blast
03/11/2013
The army hearing program
Heritage of army audiology and the road ahead: The Army Hearing Program
Mc Ilwain DS et all. Am J Public Health. 2008;98:2167–2172
Il n'y a pas que le PTSD qui soit considéré comme un enjeu majeur de dépistage et de traitement. La perte auditive bénéficie également d'un programme de grande ampleur au sein de l'armée américaine.
Les deux images qui suivent expliquent pourquoi:
1. La fréquence des déficits auditifs liés au combat
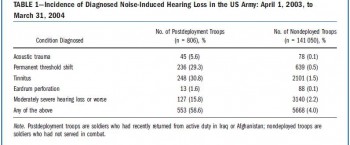
Un point détaillé récent ici
2. L'ouie est un système d'arme:
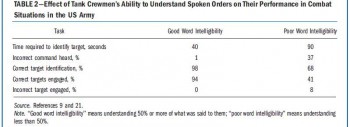
Ce document vous en décrit les grandes lignes
----------------------------------------
" Noise-induced hearing loss has been documented as early as the 16th century, when a French surgeon, Ambroise Pare´ , wrote of the treatment of injuries sustained by firearms and described acoustic trauma in great detail. Even so, the protection of hearing would not be addressed for three more centuries, when the jet engine was invented and resulted in a long overdue whirlwind of policy developmentaddressingtheprevention of hearing loss. We present a synopsis of hearing loss prevention in the US Army and describe the current Army Hearing Program, which aims to prevent noise-induced hearing loss in soldiers and to ensure their maximum combat effectiveness.............
With hearing conservation programs documenting marked initial improvements, the anticipated cost of veterans’ disability claims and payments were expected to decrease over time.10,11 However, with the start of the war in Afghanistan in 2001 and the war in Iraq in 2003, this proved not to be the case. Current data show that 51.8% of combat soldiers have moderately severe hearing loss or worse, mainly because of the loud sounds associated with combat. The implications for the army are great. When soldiers reach these levels of hearing loss, they must be evaluated for the ability to perform their duties safely and effectively. Depending on the findings, they may be given the option of changing to a job that does not put their hearing at further risk or leaving the service with a medical discharge......
."
| Tags : blast
02/11/2013
Blast et audition: Le responsable ?
Mechanisms of Hearing Loss after Blast Injury to the Ear
Cho S. et All. Plos One 8(7): e67618. doi:10.1371/journal.pone.0067618
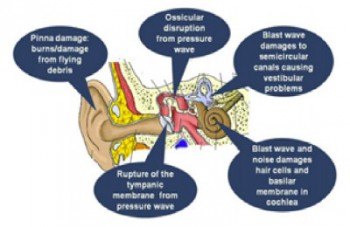
Given the frequent use of improvised explosive devices (IEDs) around the world, the study of traumatic blast injuries is of increasing interest. The ear is the most common organ affected by blast injury because it is the body’s most sensitive pressure transducer. We fabricated a blast chamber to re-create blast profiles similar to that of IEDs and used it to develop a reproducible mouse model to study blast-induced hearing loss. The tympanic membrane was perforated in all mice after blast exposure and found to heal spontaneously. Micro-computed tomography demonstrated no evidence for middle ear or otic capsule injuries; however, the healed tympanic membrane was thickened. Auditory brainstem response and distortion product otoacoustic emission threshold shifts were found to be correlated with blast intensity. As well, these threshold shifts were larger than those found in control mice that underwent surgical perforation of their tympanic membranes, indicating cochlear trauma. Histological studies one week and three months after the blast demonstrated no disruption or damage to the intra-cochlear membranes. However, there was loss of outer hair cells (OHCs) within the basal turn of the cochlea and decreased spiral ganglion neurons (SGNs) and afferent nerve synapses. Using our mouse model that recapitulates human IED exposure, our results identify that the mechanisms underlying blast-induced hearing loss does not include gross membranous rupture as is commonly believed. Instead, there is both OHC and SGN loss that produce auditory dysfunction.
-----------------
Expérimentalement, La perte auditive n'est pas liée à l'atteinte du tympan mais plutôt à l'atteinte des cellules ciliées externes et du ganglion spiral de corti. L'image qui suit tirée d'un autre document vous présente les grandes causes d'atteinte de l'audition.
| Tags : blast
15/10/2013
Dehors et dedans, ce n'est pas la même chose
Primary blast lung injury prevalence and fatal injuries from explosions: Insights from postmortem computed tomographic analysis of 121 improvised explosive device fatalities
SIngleton JAG et all. J Trauma Acute Care Surg. 2013;75: S269-S274.
BACKGROUND:
Primary blast lung injury (PBLI) is an acknowledged cause of death in explosive blast casualties. In contrast to vehicle occupants following an in-vehicle explosion, the injury profile, including PBLI incidence, for mounted personnel following an external explosion has yet to be as well defined.
METHODS:
This retrospective study identified 146 cases of UK military personnel killed by improvised explosive devices (IEDs) between November 2007 and July 2010. With the permission of Her Majesty's Coroners, relevant postmortem computed tomography imaging was analyzed. PBLI was diagnosed by postmortem computed tomography. Injury, demographic, and relevant incident data were collected via the UK Joint Theatre Trauma Registry.
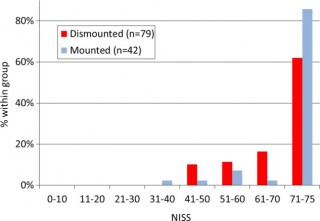
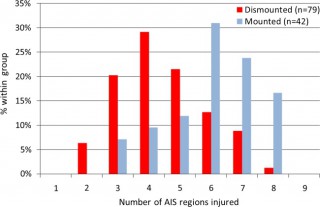
RESULTS:
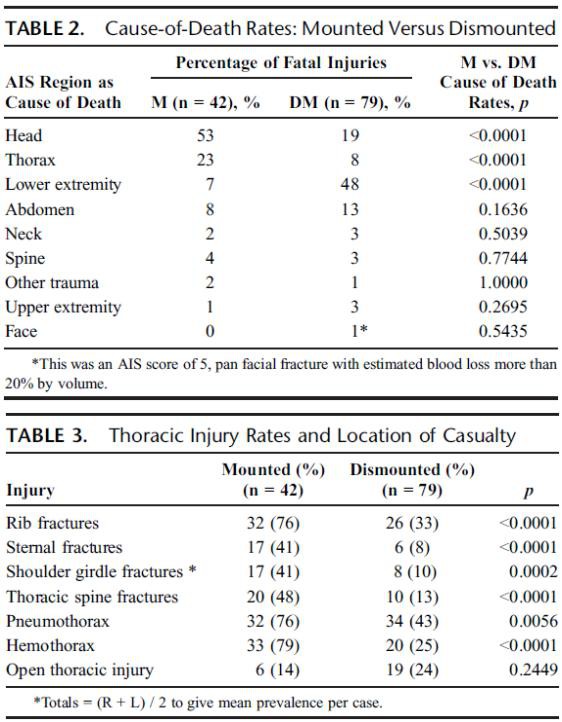
Autopsy results were not available for 1 of 146 cases. Of the remaining 145 IED fatalities, 24 had catastrophic injuries (disruptions), making further study impossible, leaving 121 cases; 79 were dismounted (DM), and 42 were mounted (M). PBLI was noted in 58 cases, 33 (79%) of 42 M fatalities and 25 (32%) of 79 DM fatalities (p < 0.0001). Rates of associated thoracic trauma were also significantly greater in the M group (p < 0.006 for all). Fatal head (53% vs. 23%) and thoracic trauma (23% vs. 8%) were both more common in the M group, while fatal lower extremity trauma (7% vs. 48%) was more commonly seen in DM casualties (p < 0.0001 for all).
CONCLUSION:
Following IED strikes, mounted fatalities are primarily caused by head and chest injuries. Lower extremity trauma is the leading cause of death in dismounted fatalities. Mounted fatalities have a high incidence of PBLI, suggesting significant exposure to primary blast. This has not been reported previously. Further work is required to determine the incidence and clinical significance of this severe lung injury in explosive blast survivors. In addition, specific characteristics of the vehicles should be considered.
| Tags : blast, balistique
07/09/2013
Blast des membres
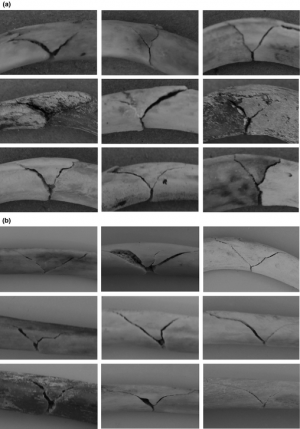
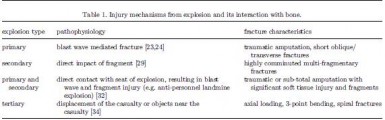
Blast-related fracture patterns: a forensic biomechanical approach
Ramasamy A. et All. J. R. Soc. Interface (2011) 8, 689–698
Dehors et dedans, ce n'est pas la même chose
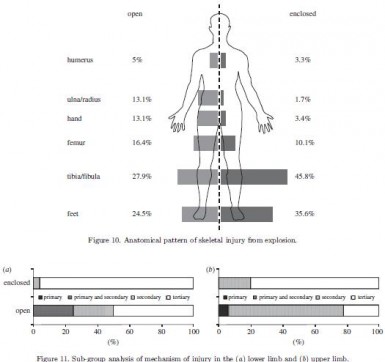
Les lésions dépendent du type de blast
| Tags : blast
Causes de DC évitables: Actualisation UK
Identifying future ‘unexpected’ survivors: a retrospective cohort study of fatal injury patterns in victims of improvised explosive devices
To identify potentially fatal injury patterns in explosive blast fatalities in order to focus research and mitigation strategies, to further improve survival rates from blast trauma.
DESIGN:
Retrospective cohort study.
PARTICIPANTS:
UK military personnel killed by improvised explosive device (IED) blasts in Afghanistan, November 2007-August 2010.
SETTING:
UK military deployment, through NATO, in support of the International Security Assistance Force (ISAF) mission in Afghanistan.
DATA SOURCES:
UK military postmortem CT records, UK Joint Theatre Trauma Registry and associated incident data.
MAIN OUTCOME MEASURES:
Potentially fatal injuries attributable to IEDs.
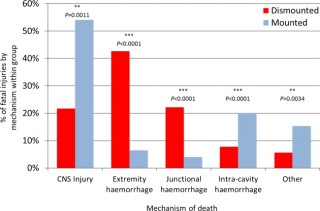
RESULTS:
We identified 121 cases, 42 mounted (in-vehicle) and 79 dismounted (on foot), at a point of wounding. There were 354 potentially fatalinjuries in total. Leading causes of death were traumatic brain injury (50%, 62/124 fatal injuries), followed by intracavity haemorrhage (20.2%, 25/124) in the mounted group, and extremity haemorrhage (42.6%, 98/230 fatal injuries), junctional haemorrhage (22.2%, 51/230 fatal injuries) and traumatic brain injury (18.7%, 43/230 fatal injuries) in the dismounted group.
CONCLUSIONS:
Head trauma severity in both mounted and dismounted IED fatalities indicated prevention and mitigation as the most effective strategies to decrease resultant mortality. Two-thirds of dismounted fatalities had haemorrhage implicated as a cause of death that may have been anatomically amenable to prehospital intervention. One-fifth of the mounted fatalities had haemorrhagic trauma which currently could only be addressed surgically. Maintaining the drive to improve all haemostatic techniques for blast casualties, from point of wounding to definitive surgical proximal vascular control, alongside the development and application of novel haemostatic interventions could yield a significant survival benefit. Prospective studies in this field are indicated.
Cette publication est très importante car elle insiste sur l'absolue nécessité de poursuivre les efforts en vue de prévenir le trauma aussi bien en matière de protection balistique, de réduction des délais de transports pour permettre la prise en charge d'hémorragie intra-cavitaires et l'aspect fondamental d'arrêter toutes les hémorragies sur le terrain notamment pas la mise en oeuvre d'une nouvelle catégorie de garrots pour les hémorragies jonctionnelles (voir 1, 2, 3, 4, 5, 6)
Les morts par IED sont plus sévèrement atteints dans un véhicule qu'à pied.
58% des Décès sont liés à plus de 2 causes potentiellement évitables
Les causes de décès ne sont pas les mêmes en combat à pied ou en véhicule
| Tags : balistique, blast, traumatologie, explosion, jonctionnel
26/03/2013
Mesurer l'exposition au blast: Une réalité
La nécessité de connaître le niveau d'exposition à une onde de blast commence à devenir évidente.Des dispositifs adaptés appraissent sur le marché. Parmi ceux ci le BLAST GAUGE semble intéressant. Porté sur le casque, le gilet pare-balle ou tout autre surface il enregistre l'onde de pression, permet la reconnaissance du niveau par led colorée et l'analyse de la courbe par récupération des données sur un ordinateur.
Le dispositif
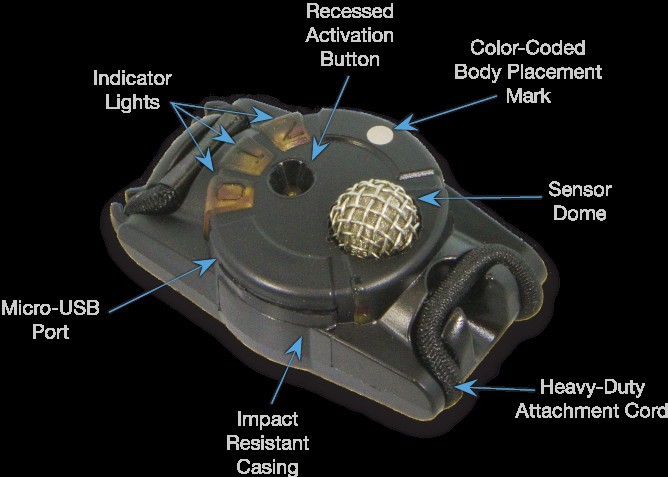
Port sur le casque

D'autres systèmes sont proposés comme le système HEADS de la société BAE dont près de 20 000 dispositfs ont été fournis à l'amée américaine et il est hautement propable que ce type de ce produit va très rapidement être mis en oeuvre dès lors qu'une expsoition à de fortes explosions notamment en milieu clos est attendue.
| Tags : blast, balistique
18/02/2012
Exposition répétées: Plus graves ! ou ?
Primary blast survival and injury risk assessment for repeated blast exposures
Panzer MB et all. J Trauma. 2012;72: 454–466.
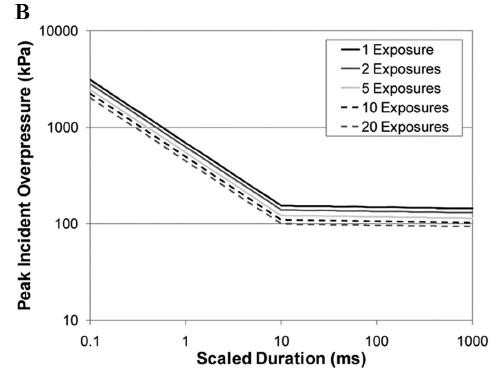
Les conflits afghnas et irakiens ont vu les personnels des armées occidentales confrontées à de nouvelles modalités d'exposition à des ondes de surpression. Leur caractèes répété est responsable de lésions plus graves. Cet article actualise un certain nombre de données.
Ces quelques diagrammes expriment de manière très claire la relation entre le pic de pressions, sa durée et la répétition sur la survie et les lésions observées.
-------------------------------------------------------
BACKGROUND:
The widespread use of explosives by modern insurgents and terrorists has increased the potential frequency of blast exposure in soldiers and civilians. This growing threat highlights the importance of understanding and evaluating blast injury risk and the increase of injury risk from exposure to repeated blast effects.
METHODS:
Data from more than 3,250 large animal experiments were collected from studies focusing on the effects of blast exposure. The current study uses 2,349 experiments from the data collection for analysis of the primary blast injury and survival risk for both long- and short-duration blasts, including the effects from repeated exposures. A piecewise linear logistic regression was performed on the data to develop survival and injury risk assessment curves.
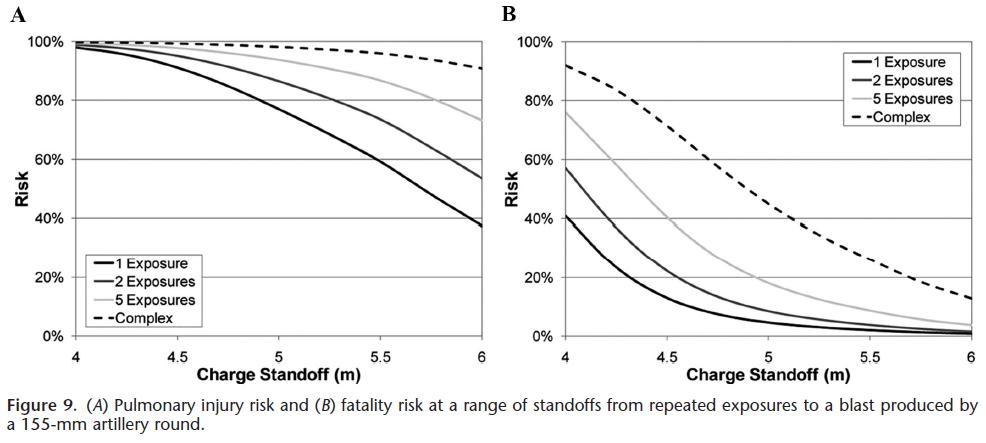
RESULTS:
New injury risk assessment curves uniting long- and short-duration blasts were developed for incident and reflected pressure measures and were used to evaluate the risk of injury based on blast overpressure, positive-phase duration, and the number of repeated exposures. The risk assessments were derived for three levels of injury severity: nonauditory, pulmonary, and fatality. The analysis showed a marked initial decrease in injury tolerance with each subsequent blast exposure. This effect decreases with increasing number of blast exposures.
CONCLUSIONS:
The new injury risk functions showed good agreement with the existing experimental data and provided a simplified model for primary blast injury risk. This model can be used to predict blast injury or fatality risk for single exposure and repeated exposure cases and has application in modern combat scenarios or in setting occupational health limits.
-------------------------------------------------------

05/12/2011
Audition du combattant et blast
Ear injuries sustained by British service personnel subjected to blast trauma
Breeze J. et all. The Journal of Laryngology & Otology (2011), 125, 13–17
Objectives:
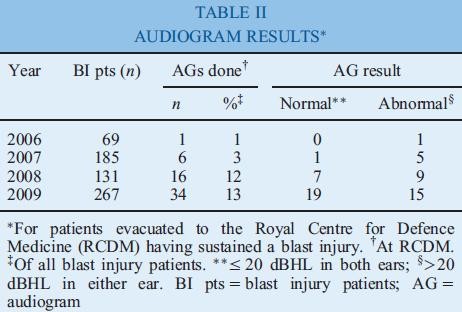
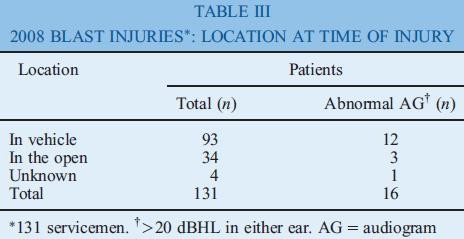
To describe the pattern of ear injuries sustained by all British servicemen serving in Iraq and Afghanistan between 2006 and 2009; to identify all servicemen evacuated to the Royal Centre for Defence Medicine following blast injury; to ascertain how many underwent otological assessment; and to calculate the incidence of hearing loss.
Design and setting:
A retrospective analysis of data obtained from the Joint Theatre Trauma Registry and the Defence Analytical and Statistics Agency, together with audiometry records from the University Hospitals Birmingham National Health Service Trust.
Results:
Ear damage was present in 5 per cent of all British servicemen sustaining battle injuries. Tympanicmembrane rupture occurred in 8 per cent of personnel evacuated with blast injuries. In 2006, 1 per cent of servicemen sustaining blast injury underwent audiography; this figure rose to 13 per cent in 2009. Fifty-three per cent of these audiograms were abnormal.

Conclusion:
The incidence of tympanic membrane rupture was higher than that found in previous conflicts. Otological assessment prior to and following military deployment is required to determine the incidence of ear injury amongst British servicemen following blast trauma.