21/12/2019
En attendant le REBOA: Une paire de main ou un genou !
Proximal External Aortic Compression for Life-Threatening Abdominal-Pelvic and Junctional Hemorrhage: An Ultrasonographic Study in Adult Volunteers.
INTRODUCTION:
Following life-threatening junctional trauma, the goal is to limit blood loss while expediting transfer to operative rescue. Unfortunately, life-threatening abdominal-pelvic or junctional hemorrhage is often not amenable to direct compression and few temporizing strategies are available beyond hemostatic dressings, hypotensive resuscitation, and balanced transfusion.
OBJECTIVES:
In this study, we evaluated proximal external aortic compression to arrest blood flow in healthy adult men.
METHODS:
This was a simulation trial of proximal external aortic compression, for life-threatening abdominal-pelvic and junctional hemorrhage, in a convenience sample of healthy adult male volunteers. The primary end points were cessation of femoral blood flow as assessed by pulse wave Doppler ultrasound at the right femoral artery, caudal to the inguinal ligament. Secondary end points were discomfort and negative sequelae.
RESULTS:
Aortic blood flow was arrested in 12 volunteers. Median time to blood flow cessation was 12.5 seconds. Median reported discomfort was 5 out of 10. No complications or negative sequelae were reported.

CONCLUSION:
This trial suggests that it may be reasonable to attempt temporization of major abdominal-pelvic and junctional hemorrhage using bimanual proximal external aortic compression. In the absence of immediate alternatives for this dangerous and vexing injury pattern, there appear to be few downsides to prehospital proximal external aortic compression while concomitantly expediting definite care.
01/12/2019
Quel tourniquet ?: Cela évolue, un peu
| Tags : tourniquet
14/10/2019
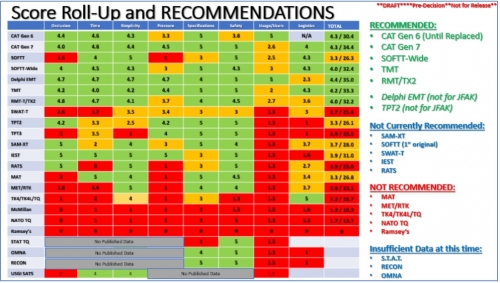
Pansements compressifs: Le test de la NAMRU
Pas nouveau mais instructif dans le contexte de bataille commerciale entre les industriels
08/10/2019
IT Clamp: Pas convaincant !
External Soft-Tissue Hemostatic Clamp Compared to a Compression Tourniquet as Primary Hemorrhage Control Device in Pilot Flow Model Study.
INTRODUCTION:
Acute blood loss represents a leading cause of death in both civilian and battlefield trauma, despite the prioritization of massive hemorrhage control by well-adopted trauma guidelines. Current Tactical Combat Casualty Care (TCCC) and Tactical Emergency Casualty Care (TECC) guidelines recommend the application of a tourniquet to treat life-threatening extremity hemorrhages. While extremely effective at controlling blood loss, the proper application of a tourniquet is associated with severe pain and could lead to transient loss of limb function impeding the ability to self-extricate or effectively employ weapons systems. As a potential alternative, Innovative Trauma Care (San Antonio, Texas USA) has developed an external soft-tissue hemostatic clamp that could potentially provide effective hemorrhage control without the aforementioned complications and loss of limb function. Thus, this study sought to investigate the effectiveness of blood loss control by an external soft-tissue hemostatic clamp versus a compression tourniquet.
HYPOTHESIS:
The external soft-tissue hemostatic clamp would be non-inferior at controlling intravascular fluid loss after damage to the femoral and popliteal arteries in a normotensive, coagulopathic, cadaveric lower-extremity flow model using an inert blood analogue, as compared to a compression tourniquet.
METHODS:
Using a fresh cadaveric model with simulated vascular flow, this study sought to compare the effectiveness of the external soft-tissue hemostatic clamp versus the compression tourniquet to control fluid loss in simulated trauma resulting in femoral and posterior tibial artery lacerations using a coagulopathic, normotensive, cadaveric-extremity flow model. A sample of 16 fresh, un-embalmed, human cadaver lower extremities was used in this randomized, balanced two-treatment, two-period, two-sequence, crossover design. Statistical significance of the treatment comparisons was assessed with paired t-tests. Results were expressed as the mean and standard deviation (SD).
RESULTS:
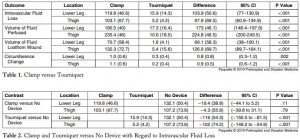
Mean intravascular fluid loss was increased from simulated arterial wounds with the external soft-tissue hemostatic clamp as compared to the compression tourniquet at the lower leg (119.8mL versus 15.9mL; P <.001) and in the thigh (103.1mL versus 5.2mL; P <.001).
CONCLUSION:
In this hemorrhagic, coagulopathic, cadaveric-extremity experimental flow model, the use of the external soft-tissue hemostatic clamp as a hasty hemostatic adjunct was associated with statistically significant greater fluid loss than with the use of the compression tourniquet.
Formation au Tourniquet: Il faut mieux faire
High Tourniquet Failure Rates Among Non-Medical Personnel Do Not Improve with Tourniquet Training, Including Combat Stress Inoculation: A Randomized Controlled Trial.
BACKGROUND:
The rate of failing to apply a tourniquet remains high.
HYPOTHESIS:
The study objective was to examine whether early advanced training under conditions that approximate combat conditions and provide stress inoculation improve competency, compared to the current educational program of non-medical personnel.
METHODS:
This was a randomized controlled trial. Male recruits of the armored corps were included in the study. During Combat Lifesaver training, recruits apply The Tourniquet 12 times. This educational program was used as the control group. The combat stress inoculation (CSI) group also included 12 tourniquet applications, albeit some of them in combat conditions such as low light and physical exertion. Three parameters defined success, and these parameters were measured by The Simulator: (1) applied pressure ≥ 200mmHg; (2) time to stop bleeding ≤ 60 seconds; and (3) placement up to 7.5cm above the amputation.
RESULTS:
Out of the participants, 138 were assigned to the control group and 167 were assigned to the CSI group. The overall failure rate was 80.33% (81.90% in the control group versus 79.00% in the CSI group; P value = .565; 95% confidence interval, 0.677 to 2.122). Differences in pressure, time to stop bleeding, or placement were not significant (95% confidence intervals, -17.283 to 23.404, -1.792 to 6.105, and 0.932 to 2.387, respectively).
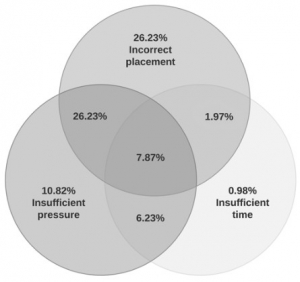
Tourniquet placement was incorrect in most of the applications (62.30%).
CONCLUSIONS:
This study found high rates of failure in tourniquet application immediately after successful completion of tourniquet training. These rates did not improve with tourniquet training, including CSI. The results may indicate that better tourniquet training methods should be pursued.
| Tags : tourniquet
21/09/2019
Garrot: Précoce, mais à réévaluer
Duration of extremity tourniquet application profoundly impacts soft-tissue antibiotic exposure in a rat model of ischemia-reperfusion injury
Mangum LC et al. Injury 10.1016/j.injury.2019.09.025
Introduction
Extremity tourniquet (TNK) application is an effective means of achieving compressible hemorrhage control in the emergency prehospital and clinical trauma setting. Modern United States military medical doctrine recommends TNK use to prevent lethal hemorrhage from extremity injury, followed by systemic prophylactic antibiotics to prevent wound infection. Because tissue pharmacokinetics of prophylactic antimicrobials during and after TNK-induced limb ischemia are largely unknown, this study was conducted to empirically determine the relationship between TNK application time and soft tissue antibiotic exposure in order to guide medical personnel in the management of extremity trauma.
Materials and Methods
Hind limbs of anesthetized male Sprague Dawley rats were exsanguinated, and ischemia maintained by a pneumatic cuff placed at the level of the mid femur on one limb; the non-ischemic contralateral limb served as comparison tissue. Systemic prophylactic antibiotics (cefazolin, moxifloxacin, or ertapenem) were administered intravenously before or after TNK release following 2 or 4 hours of ischemia with subsequent re-dosing every 12 hours for 3 days. Free antibiotic in the interstitial fluid (ISF) of the tibialis anterior muscle of both hind limbs was recovered via microdialysis during ischemia and over three periods during reperfusion: immediately following TNK release, at 24 hours post TNK release, and at 72 hours post TNK release. Plasma and ISF free drug concentrations were determined by high-performance liquid chromatography.
Results
Tourniquet application prevented delivery of prophylactic antibiotics into distal soft tissue for the duration of ischemia, and caused a profound reduction in skeletal muscle drug exposure for up to 72 hours following TNK release. A progressive decline in tissue antibiotic exposure during reperfusion was observed as TNK times increased from 2 hours to 4 hours.

The timing and severity of reduced drug distribution in post-ischemic skeletal muscle varied substantially among the three antibiotic classes evaluated.
Conclusions
Prolonged tourniquet application can significantly reduce distribution of prophylactic antibiotics into soft tissue during and after ischemia, potentially impairing prophylaxis of extremity wound infection. Our findings support the examination of alternative approaches to wound infection prophylaxis under conditions of delayed casualty evacuation when occlusive hemorrhage control measures are utilized.
06/08/2019
Garrot tactique: Oui, mais avec une réévaluation PRECOCE
Tactical tourniquet: Surgical management must be within 3 hours.
------------------------------------------
------------------------------------------
Despite longstanding controversy, tourniquets are widely used in tactical combat casualty care, with undisputed benefits for recent conflicts in Iraq and Afghanistan. Increased time delays are a particular issue in large areas, such as the Sahel-Saharan band. Complications associated with tourniquet use are predominantly related to acute ischemia with risk of amputation and ischaemia-reperfusion injury, as shown in the first clinical case. Often stated but poorly described, misuse of tourniquet and subsequent failure to interrupt arterial blood flow is also a clinical scenario that should be recognized. In the case of misuse of the tourniquet, more significant blood loss may be expected because of venous compression (« venous tourniquet », second clinical case). Early medical re-evaluation of the tourniquet is an essential component in prolonged field care. This includes reassessment of the tourniquet's ability to achieve hemostasis, abolish the downstream pulse and the relevance of the tourniquet altogether. This combat tool requires training to be successful and complications are time dependent. Tourniquet use requires appropriate application, re-evaluation and triage of wounded personnel within 3 h towards more structured surgical management.
| Tags : tourniquet
16/05/2019
PST hémostatiques: Equivalents mais bases scientifiques pauvres
Systematic review of prehospital haemostatic dressings.
INTRODUCTION:
Haemorrhage is one of the leading causes of battlefield and prehospital death. Haemostatic dressings are an effective method of limiting the extent of bleeding and are used by military forces extensively. A systematic review was conducted with the aim of collating the evidence on current haemostatic products and to assess whether one product was more effective than others.
METHODS:
A systematic search and assessment of the literature was conducted using 13 health research databases including MEDLINE and CINAHL, and a grey literature search. Two assessors independently screened the studies for eligibility and quality. English language studies using current-generation haemostatic dressings were included. Surgical studies, studies that did not include survival, initial haemostasis or rebleeding and those investigating products without prehospital potential were excluded.
RESULTS:
232 studies were initially found and, after applying exclusion criteria, 42 were included in the review. These studies included 31 animal studies and 11 clinical studies. The outcomes assessed were subject survival, initial haemostasis and rebleeding. A number of products were shown to be effective in stopping haemorrhage, with Celox, QuikClot Combat Gauze and HemCon being the most commonly used, and with no demonstrable difference in effectiveness.
CONCLUSIONS:
There was a lack of high-quality clinical evidence with the majority of studies being conducted using a swine haemorrhage model. Iterations of three haemostatic dressings, Celox, HemCon and QuikClot, dominated the studies, probably because of their use by international military forces and all were shown to be effective in the arrest of haemorrhage.
Hémorragie: Garrot, mais aussi COMPRESSION
Bleeding control in combat fields with extreme transfer time

| Tags : tourniquet
02/05/2019
Tourniquet gonflable: Un nouveau venu
Rescue Bandage TQ Inflatable Tourniquet

Un garrot développé dans le cadre de la campagne STOP THE BLEED.
Apprendre à poser un garrot: En fait, pas si simple
Can they stop the bleed? Evaluation of tourniquet application by individuals with varying levels of prior self-reported training.
McCarty et Al. Injury. 2019 Jan;50(1):10-15. doi: 10.1016/j.injury.2018.09.041.
1 garrot sur 3 posé correctement malgré une formation ad-hoc.
--------------------------------------------------------
BACKGROUND:
Application of extremity tourniquets is a central tenet of multiple national initiatives to empower laypersons to provide hemorrhage control (HC). However, the efficacy of the general population who self-report prior first-aid (FA) or HC training on individual's ability to control bleeding with a tourniquet remains unknown. Therefore, the objective of this study was to assess the effectiveness of laypeople with self-reported prior FA or HC training to control bleeding with a tourniquet.
STUDY DESIGN:
Employees of a stadium were assessed via simulation in their ability to apply a Combat Application Tourniquet. As a subgroup analysis of a larger study, participants who self-reported: 1) No prior training, 2) FA training only or 2) FA + HC training were compared. Logistic regression adjusting for age, gender, education, willingness-to-assist, and comfort level in HC was performed.
RESULTS:
317 participants were included. Compared to participants with no prior training (14.4%,n = 16/111), those with FA training only (25.2%,n = 35/139) had a 2.12-higher odds (95%CI:1.07-4.18) of correct tourniquet application while those with FA + HC (35.8%,n = 24/67) had a 3.50-higher odds (95%CI:1.59-7.72) of correct application. Participants with prior FA + HC were more willing-to-assist and comfortable performing HC than those without prior training (p < 0.05).
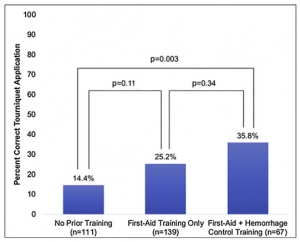
However, reporting being very willing-to-assist [OR0.83,95%CI:0.43-1.60] or very comfortable [OR1.11,95%CI:0.55-2.25] was not associated with correct tourniquet application.
CONCLUSION:
Self-reported prior FA + HC training, while associated with increased likelihood to correctly apply a tourniquet, results in only 1/3 of individuals correctly performing the skill. As work continues in empowering and training laypeople to act as immediate responders, these findings highlight the importance of effective layperson education techniques.
| Tags : tourniquet
26/04/2019
Bande de compression: Ne pas les vouer aux gémonies
Comparison of Two Tourniquets on a Mid-Thigh Model: The Israeli Silicone Stretch and Wrap Tourniquet vs. The Combat Application Tourniquet.
Le succès des garrots artériels tels que le SOFT-T et le CAT ne doit pas occulter l'intérêt des bandes de compression élastiques (Bande d'Esmach, SWAT-Tourniquet, IDF Silicone Tourniquet) préconisées en médecine rurale lors d'explosion de mines antipersonnelles (1). Ce travail met en avant leur efficacité.
-----------------------------------
Introduction:
Experience from recent conflicts underlines the dramatic impact of effective tourniquet use on combat casualty mortality. Although the Combat Application Tourniquet (CAT) is replacing the silicone band tourniquets (IST; "Israeli Silicone Tourniquet") in the Israeli Defense Forces, no direct comparison was made between them. The purpose of this study is to compare the performance of the two tourniquets on a mid-thigh model.
Methods:
Participants were Israeli military recruits who previously had the military first aid course. Each participant applied both the CAT and the IST. Applications were assessed by the HapMed Leg Tourniquet Trainer, which measured the applied pressure and the time required to reach it.

Results:
IST application resulted in higher rates of effective occlusion pressure compared with the CAT (91% vs. 73.1%, p < 0.01), and a higher mean occlusion pressure (41 mmHg, p < 0.01) was recorded using the IST. Among effective attempts, application time did not differ significantly between the tourniquets.
Effect of Elapsed Time Since First Aid Course on Success Rate
| Experience More Than 1 mo (n = 15) | Experience Equal to or Less Than 1 mo (n = 63) | p-Value | |
|---|---|---|---|
| Succeeded with CAT, n (%) | 7 (46.7) | 50 (79.4) | 0.01 |
| Succeeded with IST, n (%) | 14 (93.3) | 57 (90.5) | 0.5 |
Conclusion:
The IST was superior to the CAT in producing effective occlusion pressure while not prolonging application time. These results may indicate that the IST remains a valid option for controlling mid-thigh bleeding.
| Tags : tourniquet
04/04/2019
Un genou: Fait pour comprimer !
Martial arts technique for control of severe external bleeding.
Slevin JP et Al Emerg Med J. 2019 Mar;36(3):154-158. doi: 10.1136/emermed-2018-207966.
OBJECTIVES: Haemorrhage control is a critical component of preventing traumatic death. Other than the battlefield, haemostatic devices, such as tourniquets or bandages, may not be available, allowing for significant avoidable blood loss. We hypothesised that compression of vascular pressure points using a position adapted from the martial art of Brazilian Jiu-Jitsu could be adapted to decrease blood flow velocity in major extremity arteries.
METHODS: Knee mount compression was applied to the shoulder, groin and abdomen of healthy adult volunteer research subjects from Seattle, Washington, USA, from March through May 2018. Mean arterial blood flow velocity (MAV) was measured using ultrasound in the brachial and femoral arteries before and after compression. A MAV decrease greater than 20% with compression was deemed clinically relevant.
RESULTS: For 11 subjects, median (IQR) MAV combining all anatomical locations tested was 29.2 (34.1, 24.1) cm/s at baseline and decreased to 3.3 (0, 19.1) cm/s during compression (Wilcoxon p<0.001). MAV was significantly decreased during compression for each individual anatomical position tested (Wilcoxon p≤0.004). Per cent (95% CI) MAV reduction was significantly greater than 20% for shoulder compression at 97.5%(94% to 100%) and groin compression at 78%(56% to 100%), but was not statistically greater for abdominal compression at 35%(12% to 57%). Complete vessel occlusion was most common with compression at the shoulder (73%), followed by groin (55%) and abdomen (9%) (χ² LR, p=0.018).
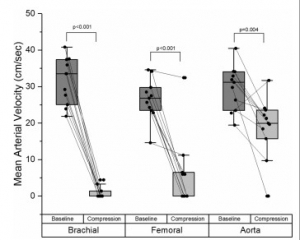
CONCLUSION: The Brazilian Jiu-Jitsu knee mount position can significantly decrease blood flow in major arteries of the extremities. This technique may be useful for bleeding control after injury.
10/03/2019
Garrot jonctionnel: Pas si performant que cela !
Comparison of Three Junctional Tourniquets Using a Randomized Trial Design.
BACKGROUND:
Hemorrhage remains a leading cause of death in both civilian and military settings. Of preventable deaths from hemorrhage, a significant portion occurs from junctional wounds that are not amenable to traditional extremity tourniquets. Junctional tourniquets (JTQs) can potentially provide hemorrhage control by compressing the arteries at the junction of the trunk and extremities. The FDA has cleared 3 JTQ products: The Combat Ready Clamp (CRoC®), the Junctional Emergency Treatment Tool (JETT™), and the SAM® JunctionalTourniquet (SJT). However, little is known regarding which of these JTQs is superior in application time, effectiveness in pulse elimination, effectiveness during transport, and user preference.
METHODS:
Active duty corpsmen (N = 49) were given standardized instruction and hands-on training with the CRoC®, JETT™, and SJT, then sequentially applied each JTQ unilaterally to a fellow study participant in a randomized order. Pulse elimination was determined by Doppler ultrasound at the dorsalis pedis immediately then reevaluated after a short transport. User preference data were collected following testing. Data were analyzed using repeated measures ANOVA and non-parametric statistics at p < 0.05.
RESULTS:
The CRoC® was significantly slower in application time than the JETT™ and SJT. Effectiveness was similar for CRoC®, JETT™, and SJT. Effectiveness during transport was significantly higher for SJT than for the JETT™, but no JTQ performed well during transport (24-48% effectiveness).
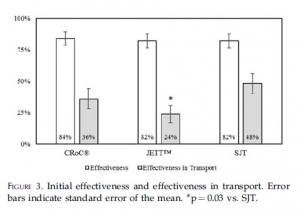
SJT ranked first in perceived ease of use, stability, and reliability, and in user trust and overall preference. Participants provided cogent suggestions for product improvement.
CONCLUSIONS:
All JTQ devices performed poorly during transport. Combined, present findings highlight the potential of JTQ products for saving lives threatened by junctional wounds, but also highlight the need for specific product improvements towards fostering JTQ performance in patient transport.
| Tags : jonctionnel
23/01/2019
Et pourquoi pas un ballonet pré-pelvien ?
Minimally invasive preperitoneal balloon tamponade and abdominal aortic junctional tourniquet versus open packing for pelvic fracture-associated hemorrhage: Not all extrinsic compression is equal.
--------------------------------------------------------
On propose souvent la réalisation d'une hémostase temporaire par a pose de sondes à ballonet. Ce travail (partiellement déjà présenté en 2016) rapporte une expérience de ce type avec un produit initialement dédié à la chirurgie pariétale herniaire. La simplicité de sa pose et son efficacité semblent prometteurs du moins chez le cochon.
--------------------------------------------------------
BACKGROUND:
Minimally invasive preperitoneal balloon tamponade (PPB) and abdominal aortic junctional tourniquets (AAJT) have been proposed as alternatives to open preperitoneal packing (OP) for the management of pelvic fracture-associated hemorrhage. We hypothesized that the PPB (SpaceMaker Pro) and AAJT would result in similar rates of survival and blood loss versus OP METHODS: 32 swine underwent creation of a combined open-book pelvic fracture and major iliac vascular injuries. Animals were randomized to no intervention (n=7), OP (n=10), PPB (n=9), or AAJT (n=6) at a mean arterial pressure <40 mmHg following initiation of uncontrolled hemorrhage. Survival (up to 60 min + 10 min after intervention reversal), hemodynamics, extraperitoneal pressures, blood loss, and associated complications were compared between groups.

RESULTS:
Prior to injury, no difference was measured between groups for weight, hemodynamics, lactate, and hematocrit (all p>0.05). The injury was uniformly lethal without intervention, with survival time (mean) of 5 min, peak preperitoneal pressure (PP) of 14 mmHg, blood loss of 960 g, and peak lactate of 2.6 mmol/L. Survival time was 44 min with OP vs. 60 min with PPB and AAJT (p<0.01). Peak PP (mmHg) was 19 with OP, 23 with PPB, and 23 with AAJT (p>0.05). Blood loss (g) was 850 with OP, 930 with PPB, and 600 with AAJT (p>0.05). Peak lactate (mmol/L) was 3.3 with OP, 4.3 with PPB, and 6.3 with AAJT (p<0.01). Only 33% of AAJT animals survived intervention reversal vs. 60% for OP and 67% for PPB (p<0.01). Necropsy revealed bowel/bladder injury in 50% of AAJT subjects vs. 0% in all other arms (p<0.01).
CONCLUSIONS:
PPB is a safe and potentially effective alternative to OP for the management of lethal pelvic fracture-associated hemorrhage. AAJT offers a similar survival benefit to PPB but has concerning rates of ischemia-reperfusion and compressive abdominal organ injury.
| Tags : pelvis
09/01/2019
Tourniquet: Comment sont ils testés ?
La qualité des garrots mis à disposition des combattants est très importante. On peut penser que c'est le cas avec les fabricants ayant pignon sur rue. C'est le cas notamment de TAC MED Solutions (SOFT Tourniquet) et de CAT Ressources ( le CAT). Il existe des machines spécifiquement conçues pour ces tests.

Clic sur l'image pour accéder au site
08/01/2019
TXA à l'avant: Peut être pas si simple !
Prehospital Tranexamic Acid Administration During Aeromedical Transport After Injury.
Tranexamic acid (TXA) has been shown to reduce mortality in the treatment of traumatic hemorrhage. This effect seems most profound when given early after injury. We hypothesized that extending a protocol for TXA administration into the prehospital aeromedical setting would improve outcomes while maintaining a similar safety profile to TXA dosed in the emergency department (ED).
MATERIALS AND METHODS:
We identified all trauma patients who received TXA during prehospital aeromedical transport or in the ED at our urban level I trauma center over an 18-mo period. These patients had been selected prospectively for TXA administration using a protocol that selected adult trauma patients with high-risk mechanism and concern for severe hemorrhage to receive TXA. Patient demographics, vital signs, lab values including thromboelastography, blood administration, mortality, and complications were reviewed retrospectively and analyzed.
RESULTS:
One hundred sixteen patients were identified (62 prehospital versus 54 ED). Prehospital TXA patients were more likely to have sustained blunt injury (76% prehospital versus 46% ED, P = 0.002). There were no differences between groups in injury severity score or initial vital signs.
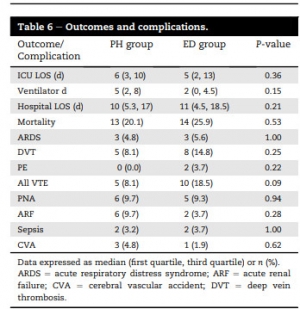
There were no differences in complication rates or mortality. Patients receiving TXA had higher rates of venous thromboembolic events (8.1% in prehospital and 18.5% in ED) than the overall trauma population (2.1%, P < 0.001).
CONCLUSIONS:
Prehospital administration of TXA during aeromedical transport did not improve survival compared with ED administration. Treatment with TXA was associated with increased risk of venous thromboembolic events. Prehospital TXA protocols should be refined to identify patients with severe hemorrhagic shock or traumatic brain injury.
09/11/2018
Tourniquet abdominal: OK pour 60 min mais max 240 min
Abdominal Aortic and Junctional Tourniquet release after 240 minutes is survivable and associated with small intestine and liver ischemia after porcine class II hemorrhage.
Uncontrolled hemorrhage is a leading cause of tactical trauma-related deaths. Hemorrhage from the pelvis and junctional regions are particularly difficult to control due to the inability of focal compression. The Abdominal Aortic and Junctional Tourniquet (AAJT) occludes aortic blood flow by compression of the abdomen. The survivability of tourniquet release beyond 120 minutes is unknown and fluid requirements to maintain sufficient blood pressure during prolonged application are undetermined. We therefore compared 60-minute and 240-minute applications and release of the AAJT for 30 minutes, with crystalloid fluid therapy, after a Class II hemorrhage.
METHODS:
Sixty-kilogram anesthetized pigs were subjected to 900-mL hemorrhage and AAJT application for 60 minutes (n = 5), 240 minutes (n = 5), and fluid therapy only for 240 minutes (n = 5) and reperfusion for 30 minutes.
RESULTS:
The AAJT application was hemodynamically and respiratory tolerable for 60 minutes and 240 minutes. Cumulative fluid requirements decreased by 64%, comparable to 3000 mL of crystalloids. Mechanical ventilation was impaired. AAJT increased the core temperature by 0.9°C compared with fluid therapy. Reperfusion consequences were reversible after 60 minutes but not after 240 minutes. A 240-minute application resulted in small intestine and liver ischemia, persisting hyperkalemia, metabolic acidosis, and myoglobinemia, suggesting rhabdomyolysis.
CONCLUSION:
The AAJT application for 240 minutes with reperfusion was survivable in an intensive care setting and associated with abdominal organ damage. Long time consequences and spinal cord effects was not assessed. We propose an application time limit within 60 minutes to 240 minutes, though further studies are needed to increase the temporal resolution. The AAJT application may be considered as a rescue option to maintain central blood pressure and core temperature in cases of hemorrhagic shock from extremity bleedings, if fluid therapy is unavailable or if the supply is limited.
08/11/2018
Tourniquet abdominal: Le - longtemps possible
Long-term consequences of abdominal aortic and junctional tourniquet for hemorrhage control
Kheirabadi BS et Al. J Surg Res. 2018 Nov;231:99-108.
BACKGROUND:
Specialized tourniquets have been deployed to the battlefield for the control of junctional/pelvic hemorrhage despite limited knowledge concerning their safety and duration of use. This study investigated long-term effects of abdominal application of the abdominal aortic and junctionaltourniquet (AAJT) in a swine survival model.
METHODS:
Anesthetized spontaneously air-breathing swine were subjected to bilateral femoral artery injuries and subsequent 40% hemorrhage. Further hemorrhage was controlled by applying the AAJT on the lower abdomen for 0 h (n = 2, controls), 1 h (n = 6), 1.5 h (n = 6), or 2 h (n = 3). Before tourniquet release, arterial injuries were repaired, and mechanical ventilation and rapid crystalloid fluid were provided for at least 5 min. Additional fluid and 500 mL autologous blood were transfused after restoring blood flow. Animals were recovered and their mobility and health monitored up to 2 wk.
RESULTS:
AAJT application occluded the infrarenal abdominal aorta and stopped bilateral groin hemorrhage with rapid reversal of hemorrhagic shock and improved cranial blood pressure. All animals including controls recovered overnight but regaining hind leg function varied among AAJT-treated groups.
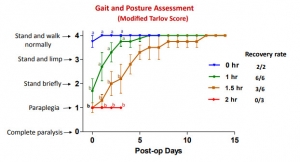
In contrast to 1 h AAJT-treated swine that recovered full mobility in 1 wk, 2 h animals developed persistent hind leg paraplegia concurrent with urinary retention and ischemic necrosis of lumber muscles and had to be euthanized 3 d after surgery. Half of the 1.5-h group also had to be euthanized early due to paraplegia, whereas the other half recovered motor function within 2 wk.
CONCLUSIONS:
The results of this animal study indicated that ischemic reperfusion injuries associated with abdominal application of the AAJT were time-dependent. To avoid permanent injuries, AAJT application on the abdomen to control a groin hemorrhage could not be longer than 1 h. This was consistent with recent instructions for application of this tourniquet on the abdomen in patients
Tourniquet abdominal = REBOA Zone 3
Comparison of zone 3 Resuscitative Endovascular Balloon Occlusion of the Aorta and the Abdominal Aortic and Junctional Tourniquet in a model of junctional hemorrhage in swine
BACKGROUND:
Traumatic injuries to the pelvis and high junctional injuries are difficult to treat in the field; however, Resuscitative EndovascularBalloon Occlusion of the Aorta (REBOA) and the Abdominal Aortic and Junctional Tourniquet (AAJT) constitute two promising treatment modalities. The aim of this study is to use a large animal model of pelvic hemorrhage to compare the survival, hemostatic, hemodynamic, and metabolic profile of both techniques.
METHODS:
Yorkshire swine (n = 10, 70-90 kg) underwent general anesthesia, instrumentation, and surgical isolation of the femoral artery. Uncontrolled hemorrhage was initiated by an arteriotomy. Animals were randomly allocated to either REBOA or AAJT. Following completion of device application, both groups received a 500 mL Hextend bolus. After 1 hour, the injured femoral artery was ligated to simulate definitive hemostasis followed by a second Hextend bolus and device removal. Animals were observed for two more hours. Physiological data were collected throughout the experiments and compared between groups.
RESULTS:
Both techniques achieved 100% hemostasis, and all animals survived the entire experiment except one in the REBOA group. During the hour treatment phase, the AAJT group had a higher mean arterial pressure than the REBOA group (59.9 ± 16.1 versus 44.6 ± 9.8 mm Hg, respectively; P < 0.05). The AAJT-treated group had higher lactate levels than the REBOA-treated group (4.5 ± 2.0 versus 3.2 ± 1.3 mg/dL, respectively; P < 0.05).
CONCLUSIONS:
Despite their mechanistic differences, both techniques achieved a similar hemostatic, hemodynamic, and metabolic profile. Some differences do exist including lactate levels and blood pressure.