----------------------------------------------------------------------------------------------------------------------
28/01/2014
Airway préhospitalier: L'approche israélienne
Prehospital intubation success rates among Israel Defense Forces providers: Epidemiologic analysis and effect on doctrine
Katzenell U. et All. J Trauma Acute Care Surg. 2013 Aug;75(2 Suppl 2):S178-83
-------------------------------------------------------------------------------------------
Un taux de succès somme toute acceptable mais par la répétition des essais. Un algorithme simple puisqu'il ne fait appel qu'à 3 techniques: l'intubation, la coniotomie et la ventilation au masque. Les auteurs recommandent de ne pas se tromper de combat et d'éviter de rentrer dans celui de l'intubation si le contexte opérationnel est très présent. Au final assez proche de ce qui est prôné dans la procédure du sauvetage au combat.
-------------------------------------------------------------------------------------------
BACKGROUND:
Advanced airway management is composed of a set of vital yet potentially difficult skills for the prehospital provider, with widely different clinical guidelines. In the military setting, there are few data available to inform guideline development. We reevaluated our advanced airway protocol in light of our registry data to determine if there were a preferred maximum number of endotracheal intubation (ETI) attempts; our success with cricothyroidotomy (CRIC) as a backup procedure; and whether there were cases where advanced airway interventions should possibly be avoided.
METHODS:
This is a descriptive, registry-based study conducted using records of the Israel Defense Forces Trauma Registry at the research section of the Trauma and Combat Medicine Branch, Surgeon General's Headquarters. We included all casualties for whom ETI was the initial advanced airway maneuver, and the number of ETI attempts was known. Descriptive statistics were used.
RESULTS:
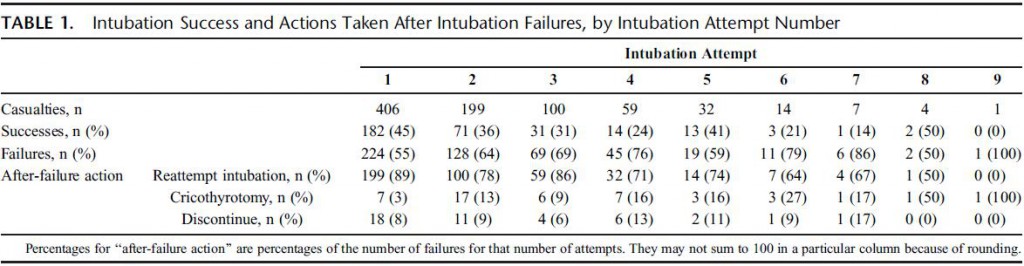
Of 5,553 casualties in the Israel Defense Forces Trauma Registry, 406 (7.3%) met the inclusion criteria. Successful ETI was performed in 317 casualties (78%) after any number of ETI attempts; an additional 46 (11%) underwent CRIC, and 43 (11%) had advanced airway efforts discontinued. ETI was successful in 45%, 36%, and 31% of the first, second, and third attempts, respectively, with an average of 28% success over all subsequent attempts. CRIC was successful in 43 (93%) of 46 casualties in whom it was attempted. Of the 43 casualties in whom advanced airway efforts were discontinued, 29 (67%) survived to hospital discharge.
CONCLUSION:
After the first ETI attempt, success with subsequent attempts tended to fall, with minimal improvement in overall ETI success seen after the third attempt. Because CRIC exhibited excellent success as a backup airway modality, we advocate controlling the airway with CRIC if ETI efforts have failed after two or three attempts. We recommend that providers reevaluate whether definitive airway control is truly necessary before each attempt to control the airway.
07/12/2013
Rupture cricotrachéale: Que faire ?
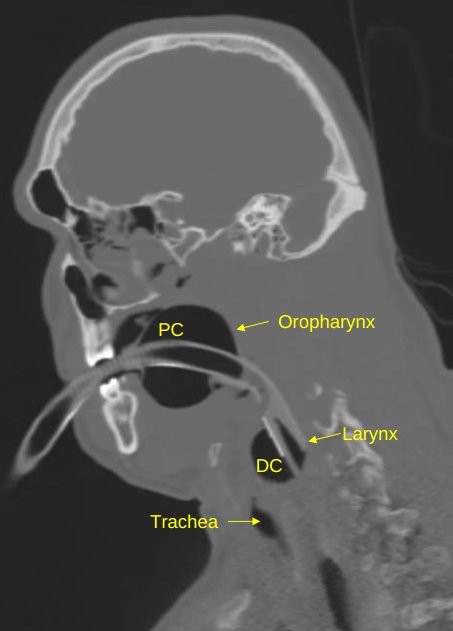
Cricotracheal Separation after Gunshot to the Neck: Report of a Survivor with Recovery of Bilateral Vocal Fold Function.
Vivero RJ et Al. http://dx.doi.org/10.1016/j.jemermed.2013.08.090
Il s'agit d'une éventualité rarissime mais cette observation montre qu'en situation d'isolement extrême il peut être possible d'agir si la partie distale est visible. Encore faut il connaître l'existence de cette conduite à tenir.
------------------------------------------------------
Initial appropriate airway management is imperative to improve survival. Numerous case reports in the literature demonstrate incidental findings of airway injury after routine workup of the patient or the advent of ominous clinical findings (1,2) . At this stage in patient management, it can become difficult to adequately secure the airway, which places the patient at increased risk. A careful physical examination is therefore critical, with fiberoptic laryngoscopy used, as necessary, in the stable patient. A CT scan can be a useful adjunct in the clinical workup, but it should not be relied upon solely, as it can be inconclusive (3) . When cricotracheal separation is identified and the patient is stable, the airway should be secured surgically in the operating room or trauma bay. The proximal stump of the airway should be grasped and secured with a clamp, and then an awake tracheotomy performed (under local anesthesia if possible) distal to the injury. In the event that the patient is unstable or that intubation fails, the distal stump of the trachea should be identified either visually or by palpation. The stump of trachea should then be grasped with a clamp and pulled superficially (out of the wound toward the skin surface), and an appropriately sized endotracheal tube is placed as a temporary measure and secured. The clamp should not be removed from the airway, as the distal tracheal stump can retract into the mediastinum. The patient should then be taken to the operating room emergently for formal tracheotomy or maturation of the airway tracheostoma. In general, cricothyrotomy should not be performed, as this is usually proximal to the site of airway separation.
| Tags : airway
06/11/2013
Voies aériennes: Avant tout une histoire de communication
Airway management: judgment and communication more than gadgets
Donati F. Can J Anesth/J Can Anesth (2013) 60:1035–1040
------------------------------------
Un éditorial publié à l'occasion de la sortie des nouvelles recommandations canadiennes sur l'intubation difficile (1 et 2). Plein de on sens et de pragmatisme et au final de rigueur scientifique dans ce document qui insiste sur le facteur humain et non le facteur matériel. . Les points essentiels sont
1. le maintien de l’oxygènation est proposé comme objectif ultime de toute manœuvre au niveau des voies aériennes
Non pas
"cannot intubate cannot ventilate"
mais
"cannot intubate cannot oxygenate"
2. Malgré la popularité croissante et l’utilisation répandue des dispositifs supraglottiques, l’intubation trachéale demeure l’étalon or et la méthode préférée pour une prise en charge stable des voies aériennes.
3. La vidéolaryngoscopie n’est pas présentée comme la solution universelle à tous les problèmes liés aux voies aériennes
4. Le nombre de tentatives, quelle que soit la technique d’intubation ou la position, devrait se limiter à trois même si n’existe aucune donnée probante solide appuyant un tel énoncé.
5. Même si il existe des données probantes selon lesquelles un accès chirurgical aux voies aériennes chirurgicales ne sauve pas toujours des vies, le groupe recommande d’essayer d’obtenir un accès chirurgical aux voies aériennes lorsque tous les autres types de tentative échouent.
29/10/2013
Intubation en préhospitalier : intérêt des nouvelles techniques
IOT difficile et les nouveaux outils en situation d’urgence ( où en est-on ? )
Les procédures validées
Combes X et All. Urgences - 2013
Points essentiels
■ L’intubation en séquence rapide est la technique de sédation validée pour faciliter l’intubation en situation d’urgence.
■ La préoxygénation peut être réalisée par VNI chez le patient coopérant.
■ Les lames de laryngoscopes en plastique ne doivent pas être utilisées.
■ L’utilisation du mandrin long béquillé est parfaitement validée en situation d’urgence en cas d’intubation difficile sans difficulté de ventilation associées.
■ Le masque laryngé d’intubation Fastrach® est le dispositif de ventilation le plus utile en situation d’urgence.
■ Les vidéolaryngoscopes ne sont pas encore validées pour la prise en charge de l’intubation difficile en situation d’urgence.
■ Les dispositifs de cricothyroïdotomiee basée sur la technique de Seldinger sont à privilégier en situation d’urgence
| Tags : airway, intubation
29/05/2013
Vidéo laryngoscopie: Du bien, on n'est pas étonné

Anesth Analg 2013;XX:XX–XX
BACKGROUND:The video laryngoscope (VL) has been shown to improve laryngoscopic views and first-attempt success rates in elective operating room and simulated tracheal intubations compared with the direct laryngoscope (DL). However, there are limited data on the effectiveness of the VL compared with the DL in urgent endotracheal intubations (UEIs) in the critically ill. We assessed the effectiveness of using a VL as the primary intubating device during UEI in critically ill patients when performed by less experienced operators.
METHODS:We compared success rates of UEIs performed by Pulmonary and Critical Care Medicine (PCCM) fellows in the medical intensive care unit and medical or surgical wards. A cohort of PCCM fellows using GlideScope VL as the primary intubating device was compared with a historical cohort of PCCM fellows using a traditional Macintosh or Miller blade DL. The primary measured outcome was first-attempt intubation success rate. Secondary outcomes included total number of attempts required for successful tracheal intubation, rate of esophageal intubation, need for supervising attending intervention, duration of intubation sequence, and incidence of hypoxemia and hypotension.
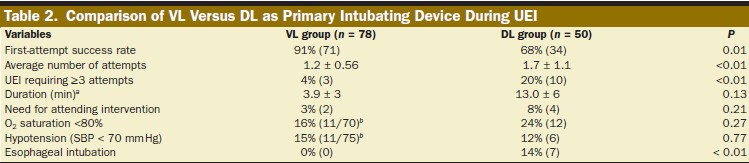
RESULTS:There were 138 UEIs, with 78 using a VL and 50 using a DL as the primary intubating device. The rate of first-attempt success was superior with the VL as compared with the DL (91% vs 68%, P < 0.01). The rate of intubations requiring ≥3 attempts (4% vs 20%, P < 0.01), unintended esophageal intubations (0% vs 14%, P < 0.01), and the average number of attempts required for successful tracheal intubation (1.2 ± 0.56 vs 1.7 ± 1.1, P < 0.01) all improved significantly with use of the VL compared with the DL.
CONCLUSIONS:UEI using a VL as the primary device improved intubation success anddecreased complications compared with a DL when PCCM fellows were the primary operators. These data suggest that the VL should be used as the primary device when urgent intubations are performed by less experienced operators.
| Tags : intubation, airway
03/03/2013
Mieux voir pour mieux intuber. Un moyen simple surtout si on débute
Retrograde Light-guided Laryngoscopy for Tracheal Intubation. Clinical Practice and Comparison with Conventional Direct Laryngoscopy
Anesthesiology 2013; 118:XXX–XXX doi: 10.1097/ALN.0b013e31828877c0.
L'intubation orotrachéale nécessite un apprentissage réel. Une cinquantaine de procédures réussies sont nécessaires pour pouvoir considérer avoir la maîtrise de ce geste. De nombreux dispositifs permettent d'augmenter le taux de réussite (bougie, stylets lumineux, dispositifs laryngés, fibroscopie, vidéolaryngoscope). Ces dernières sont cependant onéreuses et pas forcément toujours disponibles. L'illumination transtrachéale et rétrograde du plan glottique pourrait avoir une certaine utilité en améliorant la visualisation de l'orifice glottique.
--------
Compared with DL, the success rate was greater in the RLGL group for all five intubations (72% vs. 47%; rate difference, 25%; 95% CI [11.84–38.16%], P < 0.001). This was associated with a shorter time to glottic exposure (median [25th and 75th percentile]; 27 [15; 42] vs. 45 [30; 73] s, P < 0.001), shorter intubation time (66 [44; 120] vs. 120 [69; 120] s, P < 0.001), and decreased throat soreness (mean ± SD; visual analog scale, 2.1 ± 0.9 vs. 3.7 ± 1.0 cm, P = 0.001) in the RLGL group compared to the DL group.
--------

| Tags : intubation, airway
24/02/2013
Intubation: Encore une étude POUR
Comparison of Neurological Outcome between Tracheal Intubation and Supraglottic Airway Device Insertion of Out-of-hospital Cardiac Arrest Patients: A Nationwide, Population-based, Observational Study
J Emerg Med. 2013 Feb;44(2):389-97
BACKGROUND:
The effect of prehospital use of supraglottic airway devices as an alternative to tracheal intubation on long-term outcomes of patients with out-of-hospital cardiac arrest is unclear.
STUDY OBJECTIVES:
We compared the neurological outcomes of patients who underwent supraglottic airway device insertion with those who underwent tracheal intubation.
METHODS:
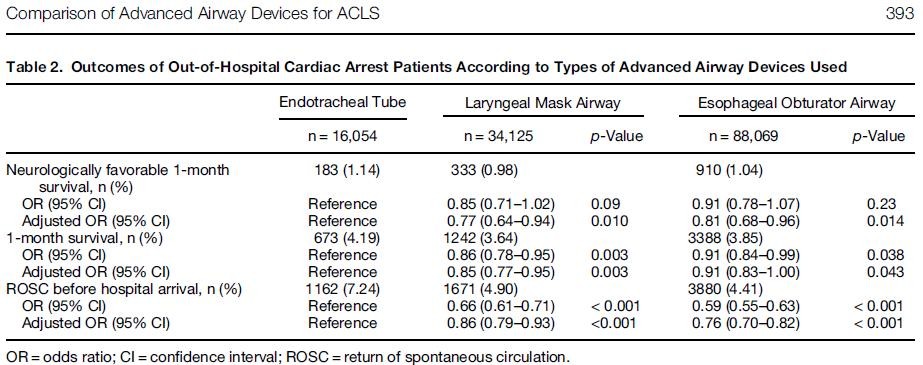
We conducted a nationwide population-based observational study using a national database containing all out-of-hospital cardiac arrest cases in Japan over a 3-year period (2005-2007). The rates of neurologically favorable 1-month survival (primary outcome) and of 1-month survival and return of spontaneous circulation before hospital arrival (secondary outcomes) were examined. Multiple logistic regression analyses were performed to adjust for potential confounders. Advanced airway devices were used in 138,248 of 318,141 patients, including an endotracheal tube (ETT) in 16,054 patients (12%), a laryngeal mask airway (LMA) in 34,125 patients (25%), and an esophageal obturator airway (EOA) in 88,069 patients (63%).
RESULTS:
The overall rate of neurologically favorable 1-month survival was 1.03% (1426/137,880). The rates of neurologically favorable 1-month survival were 1.14% (183/16,028) in the ETT group, 0.98% (333/34,059) in the LMA group, and 1.04% (910/87,793) in the EOA group. Compared with the ETT group, the rates were significantly lower in the LMA group (adjusted odds ratio 0.77, 95% confidence interval [CI] 0.64-0.94) and EOA group (adjusted odds ratio 0.81, 95% CI 0.68-0.96).
CONCLUSIONS:
Prehospital use of supraglottic airway devices was associated with slightly, but significantly, poorer neurological outcomes compared with tracheal intubation, but neurological outcomes remained poor overall.
| Tags : airway, intubation
20/08/2012
L'intubation mieux qu'un dispositif supraglottique
Endotracheal intubation versus supraglottic airway insertion in out-of-hospital cardiac arrest
Wang HE et all. Resuscitation 83 (2012) 1061–1066
-------------------------------------------------------------------
Lors de la prise en charge préhospitalière d'un arrêt cardiaque il vaut mieux intuber que mettre en place un dispositif laryngé. Les conclusions de ce travail interpellent car elles vont à l'encontre de certaines propositions d'emploi de dispositifs laryngés pour le contrôle préhospitalier des voies aériennes.
-------------------------------------------------------------------
Objective
To simplify airway management and minimize cardiopulmonary resuscitation (CPR) chest compression interruptions, some emergency medical services (EMS) practitioners utilize supraglottic airway (SGA) devices instead of endotracheal intubation (ETI) as the primary airway adjunct in out-of-hospital cardiac arrest (OHCA). We compared the outcomes of patients receiving ETI with those receiving SGA following OHCA.
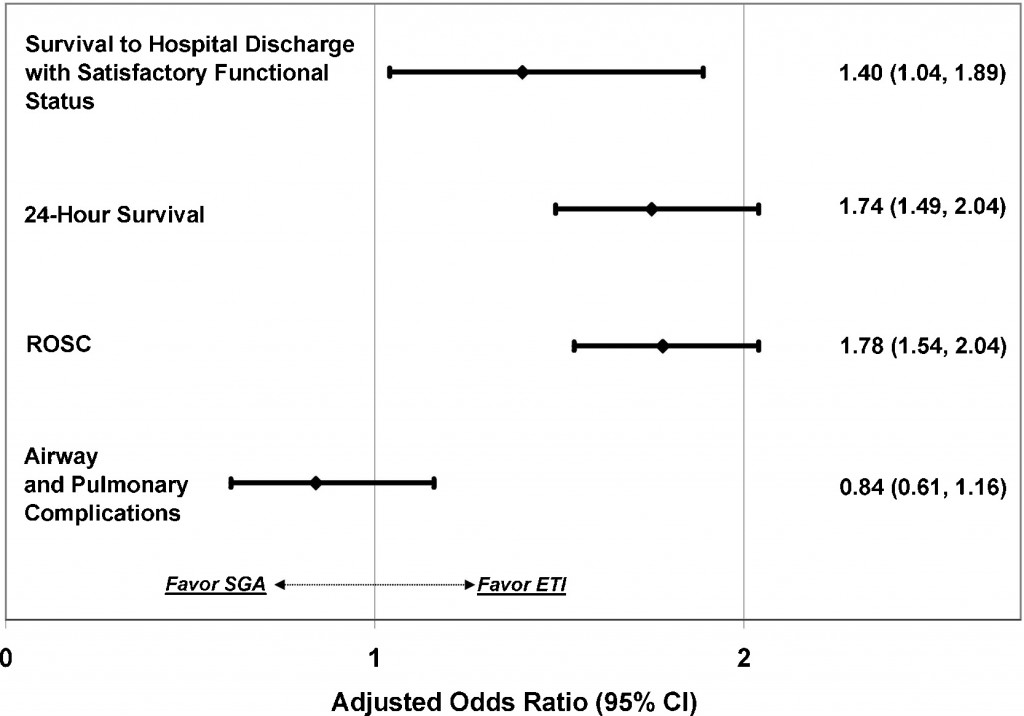
We performed a secondary analysis of data from the multicenter Resuscitation Outcomes Consortium (ROC) PRIMED trial. We studied adult non-traumatic OHCA receiving successful SGA insertion (King Laryngeal Tube, Combitube, and Laryngeal Mask Airway) or successful ETI. The primary outcome was survival to hospital discharge with satisfactory functional status (Modified Rankin Scale ≤3). Secondary outcomes included return of spontaneous circulation (ROSC), 24-h survival, major airway or pulmonary complications (pulmonary edema, internal thoracic or abdominal injuries, acute lung injury, sepsis, and pneumonia). Using multivariable logistic regression, we studied the association between out-of-hospital airway management method (ETI vs. SGA) and OHCA outcomes, adjusting for confounders.
Of 10,455 adult OHCA, 8487 (81.2%) received ETI and 1968 (18.8%) received SGA. Survival to hospital discharge with satisfactory functional status was: ETI 4.7%, SGA 3.9%. Compared with successful SGA, successful ETI was associated with increased survival to hospital discharge (adjusted OR 1.40; 95% CI: 1.04, 1.89), ROSC (adjusted OR 1.78; 95% CI: 1.54, 2.04) and 24-h survival (adjusted OR 1.74; 95% CI: 1.49, 2.04). ETI was not associated with secondary airway or pulmonary complications (adjusted OR 0.84; 95% CI: 0.61, 1.16).
In this secondary analysis of data from the multicenter ROC PRIMED trial, ETI was associated with improved outcomes over SGA insertion after OHCA.
17/07/2012
Dispositifs laryngés: Toujours pas validés !
Un retour d'expérience à méditer qui met en évidence que plus de la moitié des dispositifs laryngés posés en préhospitalier ne sont pas positionnés de manière correcte.
http://www.medicalsci.com/files/f2f__10__king_ltd_-_afmes...
Un document faisant le point sur les divers dispositifs laryngés est accessible ici
| Tags : airway
18/04/2012
Conférence Experts: Intubation difficile
| Tags : intubation
Intubation: Une vision en secours en montagne
09/12/2011
Intubation: Une formation minimale
A Critical Reassessment of Ambulance Service
Airway Management in Pre-Hospital Care
Deakin C et all.
08/09/2011
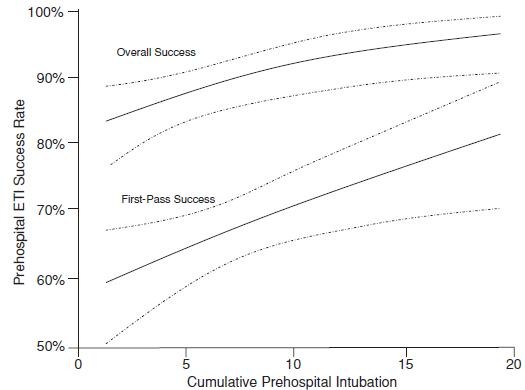
Plus on fait, mieux on réussit !
20 intubations avant d'être fiable
06/05/2011
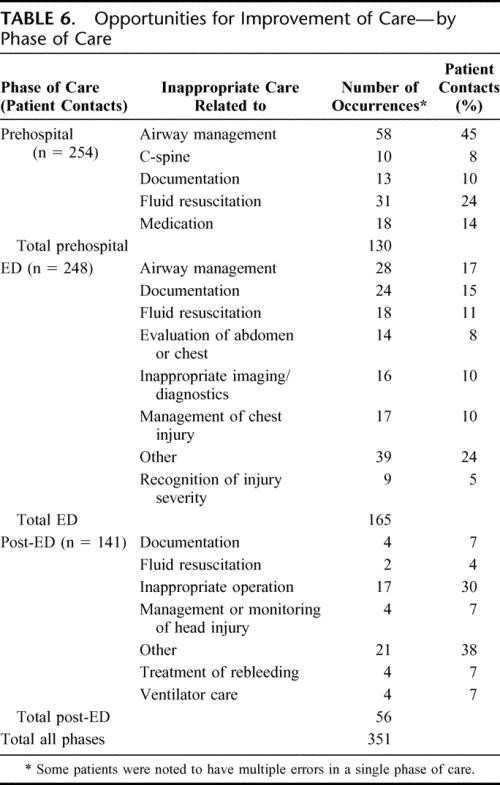
Mieux maîtriser les voies aériennes: Un axe majeur pour réduire la motalité préhospitalière du traumatisé
Analysis of Preventable Trauma Deaths and Opportunities for Trauma Care Improvement in Utah
15/02/2011
Intubation préhospitalière: Que penser de l'AIRTRAQ ?
Comme pour tout il faut s'entraîner et on n'inove pas. On rappelle que, en conditions de combat, le contrôle des voies aériennes a pour but essentiellemment de prévenir l'obstruction des voies aériennes, de prévenir l'inhalation du contenu gastrique. Le traitement d'une détresse respiratoire fait appel avant tout à l'oxygénothérapie si vous disposez d'oxygène, au traitement d'une cause spécifique (pneumo ou hémothorax, volet thoracique, plaie soufflante), à l'assistance ventilatoire au ballon par masque facial et EVENTUELLEMENT après intubation ou coniotomie sur une canule de 6 mm si les conditions tactiques le permettent.
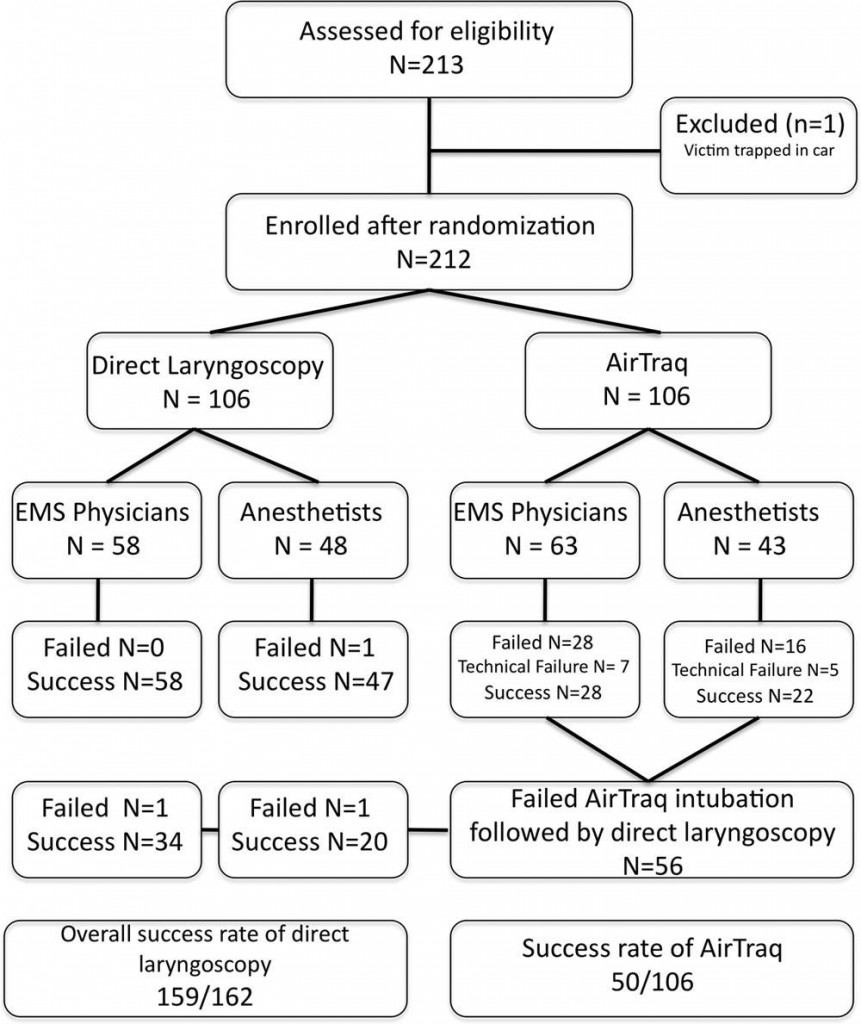
Use of the Airtraq laryngoscope for emergency intubation in the prehospital setting: A randomized control trial
Trimmel H et all.
Crit Care Med 2011 Vol. 39, No. 3, 1-5
Objectives: The optical Airtraq laryngoscope (Prodol Meditec, Vizcaya, Spain) has been shown to have advantages when compared with direct laryngoscopy in difficult airway patients. Furthermore, it has been suggested that it is easy to use and handle even for inexperienced advanced life support providers. As such, we sought to assess whether the Airtraq may be a reliable alternative to conventional intubation when used in the prehospital setting.
Design, Setting, and Patients: Prospective, randomized control trial in emergency patients requiring endotracheal intubation provided by anesthesiologists or emergency physicians responding with an emergency medical service helicopter or ground unit associated with the Department of Anesthesiology, General Hospital, Wiener Neustadt, Austria.
Measurements and Main Results: During the 18-month study period, 212 patients were enrolled. When the Airtraq was used as first-line airway device (n = 106) vs. direct laryngoscopy (n =106), success rate was 47% vs. 99%, respectively (p < .001). Reasons for failed Airtraq intubation were related to the fiberoptic characteristic of this device (i.e., impaired sight due to blood and vomitus, n = 11) or to assumed handling problems (i.e., cuff damage, tube misplacement, or inappropriate visualization of the glottis, n = 24). In 54 of 56 patients where Airtraq intubation failed, direct laryngoscopy was successful on the first attempt; in the remaining two and in one additional case of failed direct laryngoscopy, the airway was finally secured employing the Fastrach laryngeal mask. There was no correlation between success rates and body mass index, age, indication for airway management, emergency medical service unit, or experience of the physicians.
Conclusions: Based on these results, the use of the Airtraq laryngoscope as a primary airway device cannot be recommended in the prehospital setting without significant clinical experience obtained in the operation room. We conclude that the clinical learning process of the Airtraq laryngoscope is much longer than reported in the anesthesia literature.
| Tags : intubation, airway
05/02/2011
Etude NEMESIS: Out-of-hospital airway management in the United States
Un travail prospectif recensant toutes les manoeuvres de contrôle des voies aériennes aux USA vient d'être publié ( Out-of-hospital airway management in the United States - Wang HE et all. -doi:10.1016/j.resuscitation.2010.12.014). Ce document est intéressant car il confirme que l'intubation est le mode premier de contrôle de la ventilation aux USA suivi par la ventilation manuelle au ballon. Le recours à des disposiifs laryngés ne vient qu'au 4ème rang après la mise en oeuvre de technqiues de ventilation non invasive. L'apprentissage de l'intubation reste donc un objectif essentiel. Les tableaux suivant en présentent les principaux résultats.

Table 1. Prevalence of airway management interventions. Table includes only EMS agencies reporting at least one procedure in the NEMSIS 2008 data set. Percentages reflect portion of 2,333,254 total patient care events. Prevalence estimates not calculated for King LT and foreign body removal due to the small numbers of events. BiPAP = bilevel positive airway pressure. CPAP = continuous positive airway pressure. PEEP = positive end expiratory pressure.
| Intervention | N | (N per 100,000 care events; 95%CI) |
|---|---|---|
| Bag-valve-mask ventilation | 8809 | (378; 370–386) |
| Other ventilation (bag-valve, mechanical, unspecified) | 12,241 | (525; 516–534) |
| Endotracheal intubation | 10,356 | (444; 436–453) |
| Orotracheal intubation | 9130 | (392; 384–400) |
| Nasotracheal intuabtion | 1064 | (46; 43–48) |
| Rapid sequence intubation | 371 | (16; 14–18) |
| Alternate airway | 2246 | (96; 92–100) |
| Combitube | 1521 | (65; 62–69) |
| Esophageal-Obturator Airway (EOA) | 175 | (8; 6–9) |
| Laryngeal Mask Airway | 571 | (24; 23–27) |
| King LT | 4 | (Not calculated) |
| Cricothyroidotomy | 88 | (4; 3–5) |
| BiPAP/CPAP | 4456 | (191; 186–197) |
| Oropharyngeal airway | 4623 | (198; 193–204) |
| Nasopharyngeal airway | 37,298 | (160; 158–161) |
| Colorimetric tube confirmation | 7007 | (300; 294–308) |
| Bulb tube confirmation | 646 | (28; 26–30) |
| Nebulizer | 12,796 | (549; 539–558) |
| PEEP | 2614 | (112; 108–117) |
| Suction | 8115 | (348; 341–356) |
| Foreign body removal | 1 | (Not calculated) |
----------------------------------------------------------------------------------------------------------------------
Table 3. Airway intervention success. Includes only orotracheal, nasotracheal and rapid sequence intubation and alternate airway insertions where procedural success was reported. ETI success was reported for only 8418 of 10,356 ETI.
ETI = endotracheal intubation. US = United States.
a Subgroups do not add up to total because of unknown cardiac arrest status for 5244 cases. Univariable odds ratios presented for selected comparisons only.
----------------------------------------------------------------------------------------------------------------------
Abstract
-----Among 4,383,768 EMS activations, there were 10,356 ETI, 2246 alternate airways, and 88 cricothyroidotomies. ETI success rates were: overall 6482/8418 (77.0%; 95% CI: 76.1–77.9%), cardiac arrest 3494/4482 (78.0%), non-arrest medical 616/846 (72.8%), non-arrest injury 417/505 (82.6%), children <10 years 295/397 (74.3%), children 10–19 years 228/289 (78.9%), adult 5829/7552 (77.2%), and rapid-sequence intubation 289/355 (81.4%). ETI success was success was lowest in the South US census region. Alternate airway success was 1564/1794 (87.2%). Major complications included: bleeding 84 (7.0 per 1000 interventions), vomiting 80 (6.7 per 1000) and esophageal intubation 12 (1.0 per 1000).
Conclusions
In this study characterizing out-of-hospital airway management across the United States, we observed low out-of-hospital ETI success rates. These data may guide national efforts to improve the quality of out-of-hospital airway management.
| Tags : airway, intubation
31/12/2010
Intubation préhospitalière: Histoire de lame
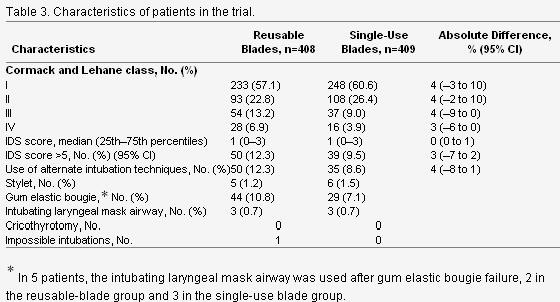
Un article d Jabre et all décrit de manière relativement précise le quotidien de l'intubation préhospitalière
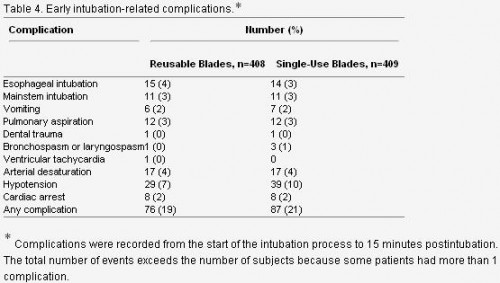
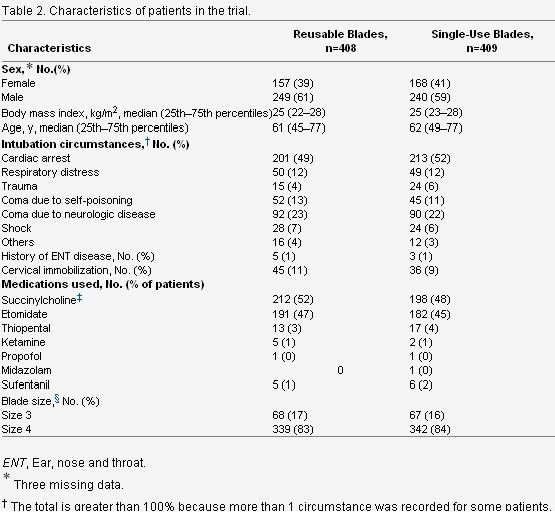
Out-of-Hospital Tracheal Intubation With Single-Use Versus Reusable Metal Laryngoscope Blades: A Multicenter Randomized Controlled Trial -
Cet article est très intéressant car il permet d'avoir une vision très claire de l'intubation telle qu'elle est réalisée en préhospitalier en France. L'objectif premier était de comparer l'intubation avec lame métallique réutilisable versus non réutilisable et de voir si il y avait une différence en matière d'intubation difficile. Ce n'est pas le cas. Parmi les autres intérêts de ce travail:
-
l'intubation préhospitalière est réalisée essentiellement lors de la prise en charge d' arrêt cardiaque ou de coma. Le contexte traumatique n'est présent que dans 4% des cas. Ce qui ne correspond pas au contexte d'emploi militaire. Le contrôle des voies aériennes ayant pour objectif essentiel le maintien de la liberté des voies aériennes, puis leur protection contre l'inhalation et enfin la possibilité de réaliser une ventilation contrôlée si les autres paramètres techniques sont accessibles (matériel, oxygène, sédation)
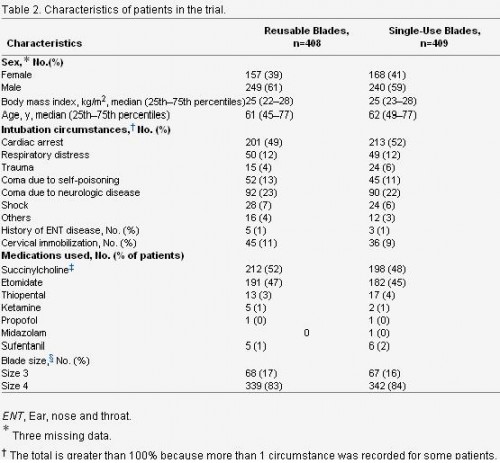
2. La taille de la lame utilisée est une taille 4. Le laryngoscope Truphatek Trulite en dotation est approvisionné en taille 3. Ceci a été jugé suffisant par un panel de praticiens, ce d'autant que les lames de tailles 4 sont aussi plus hautes et pas forcément toujours « insérables » dans la cavité buccale en cas de petite ouverture de bouche.
3. Le recours à des techniques alternatives est prévu, ici le masque laryngé d'intubation qui est utilisé de manière exceptionnelle moins de 1% des cas, contrairement au mandrin d'eschmann/Frova.
4. Parmi les complications immédiates, on constate la fréquence des hypotensions près de 10% et des intubations sélectives ou oesophagiennes également près de 10% des cas. Ces taux observés pour des équipes à priori entraînées illustrent bien que l'enjeu majeur de la médicalisation de l'avant dans le contexte actuel est de disposer de personnel ayant une pratique réelle de l'accès aux voies aériennes supérieures.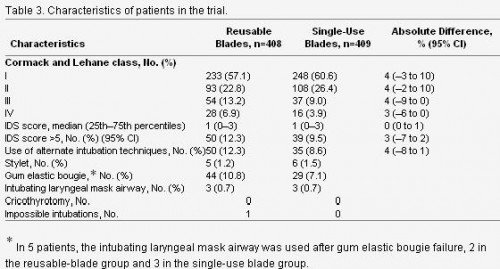

| Tags : intubation, airway
17/12/2010
Quel laryngoscope ?
Le choix d'un laryngoscope "tactique" n'est pas simple. C'est un compromis entre la modalité choisie de contrôle des voies aériennes (pas d'intubation, coniotomie ou intubation ?), le poids du laryngoscope, la taille de la lame et les qualités optiques attendues.
Vous dispsoez outre de la boite d'intubation standard du laryngoscope trulite de la société truphatek.

Il a été choisi d'approvionner ce laryngoscope en lame fixe de taille 3 qui semble la plus polyvalente. Ce laryngoscope est remarquable de part sa légèreté, la présence d'un manche court et la qualité de la lumière LED fournie. Il est en principe à patient unique.
Pour pallier au problème du choix de la taille de la lame, certains proposent des produits originaux. Ainsi le duoscope de la société PARKER propose deux tailles de lame et un éclairage de grande qualité. sa manipulation est moins aisée car c'est la seconde lame qui sert de manche.
| Tags : intubation, airway
14/12/2010
Abord des voies aériennes:Que font les anglais ?
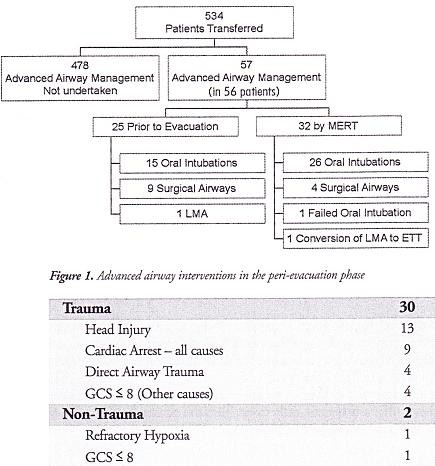
10 % des blessés évacués nécessite une intubation dont 4.7% avant l'embarquement dans le vecteur d'évacuation. Dans ce travail la limite est que nous ne savons pas ce qui relève de blessés au combat , s'il s'agit de blessés militaires, de la répartition des procédures en fonction du contexte. Dans de telles conditions la prise en charge de patients/blessés en arrêt circulatoire est vaine .
J R Army Med Corps. 2010 Sep;156(3):159-61.
Advanced airway management--a medical emergency response team perspective.
Selly Oak Hospital, Birmingham. aghaldane1@doctors.org.uk
Abstract
OBJECTIVES: To determine the number of medical emergency response team (MERT) patients undergoing advanced airway management in the peri-evacuation phase and to determine the indications for airway interventions undertaken in flight.
METHODS: This was a retrospective study. Data was collected from patient report and mission debrief forms completed after each MERT mission during Operation HERRICK 10 (April-October 2009). All patients that received advanced airway interventions before or during evacuation were identified.
RESULTS: MERTs were involved in the primary transfer of 534 patients during the period studied, 56 (10.5%) underwent advanced airway management, of which 31 (5.8% of total) were initiated by the MERT in the peri-evacuation phase. Twenty five cases (4.7%) underwent advanced airway management by other pre-hospital providers prior to MERT arrival. Of the 31 advanced airway interventions undertaken in-flight, cardiac arrest was the primary indication in only nine cases.
CONCLUSIONS: The figure of 56 patients requiring advanced airway management is at the higher end of the range expected from the study of historical military data. This may reflect the doctrine of "intelligent tasking", that is sending this physician-led team to the most seriously injured casualties.
Morceaux choisis
1. Intubation et coniotomie sont la base
2. Les indications diffèrent de la médecine préhospitalière civile
"..
The indications for those advanced airway interventions undertaken by the MERT is in keeping with the historical data: Head injury making the biggest group once those inrubated for post-operative resplratory support ie those transferred post-operatively from an FST location rather than direct from the point of wounding are excluded . The majoriry of the cases were trauma (93,5%) with the remaining non-traula causes (6,5%) (table 1); This figure is again similar io the recent US study [11].
.."
| Tags : airway, intubation
12/12/2010
Anesthésie pour intuber: Maj des recommandations
Les dernières recommendations portant sur la sédation préhospitalière ont été publiées. L'algorithme suivant est proposé.

1. Remplacez simplement l'ephédrine par de l'adrénaline titrée (1 mg/10 ml, ml par ml pour obtenir un pouls radial perçu).
2. Notez l'emploi de l'AL de glotte
3. Notez le caractère impératif de la sédation après intubation. Cependant il n'y a pas de recommandations fortes concernant le choix midazolam/morphinique ou kétamine/morphinique. Le recours au GammaOH a été proposé en conditions de combat car ne nécessitant qu'une injection IV.