07/01/2015
Gonflez le ballonnet à l'eau et échographiez le au niveau de la fourchette sternale !
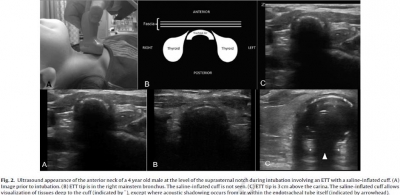
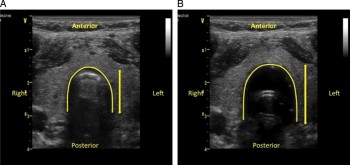
Tracheal rapid ultrasound saline test (T.R.U.S.T.) for confirming correct endotracheal tube depth in children
Tessaro MO et Al. Resuscitation. 2014 Sep 17. pii: S0300-9572(14)00741-2
------------------------------------------------------------------------------------
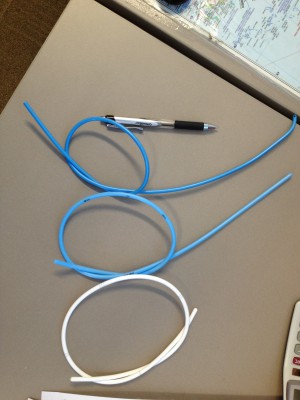
On parle beaucoup de l'apport de l'échographie en préhospitalier et plus particulièrement de l'échographie des voies aériennes. Ce travail réalisé dans un contexte de pédiatrie hospitalière est intéressant car il peut peut-être être transposé à nos besoins. Etre rapidement certain du caractère effectif de l'intubation peut être difficile. L'échographie peut être d'un apport important par la visualisation d'un glissement pleural bilatéral. On peut aussi gonfler le ballonnet de la sonde [Ce qui est fait lors de transports aériens non ou mal préssurisés], ce qui permettra d'observer non un cône d'ombre en arriere du ballonnet mais les structures anatomiques du fait de la transmissions des ondes permise par l'eau présente dans le ballonnet.
------------------------------------------------------------------------------------
OBJECTIVES:
We evaluated the accuracy of tracheal ultrasonography of a saline-inflated endotracheal tube (ETT) cuff for confirming correct ETT insertion depth.
METHODS:
We performed a prospective feasibility study of children undergoing endotracheal intubation for surgery. Tracheal ultrasonography at the suprasternal notch was performed during transient endobronchial intubation and inflation of the cuff with saline, and with the ETT at a correct endotracheal position. Ultrasound videos were recorded at both positions, which were confirmed by fiberoptic bronchoscopy. These videos were shown to two independent blinded reviewers, who determined the presence or absence of a saline-inflated cuff. The primary outcome was accuracy of tracheal ultrasonography for appropriate ETT insertion depth.
RESULTS:
Forty-two patients were enrolled. For correct endotracheal versus endobronchial positioning, pooled results from the reviewers revealed a sensitivity of 98.8% (95% CI=90-100%), a specificity of 96.4% (95% CI=87-100%), a PPV of 96.5% (95% CI=87-100%), a NPV of 98.8% (95% CI=89-100%), a positive likelihood ratio of 32 (95% CI=6-185), and a negative likelihood ratio of 0.015 (95% CI=0.004-0.2). Agreement between reviewers was high (kappa co-efficient=0.93; 95% CI=0.86 to 1). The mean duration of the ultrasound exam was 4.0s (range 1.0-15.0s).
CONCLUSIONS:
Sonographic visualization of a saline-inflated ETT cuff at the suprasternal notch is an accurate and rapid method for confirming correct ETT insertion depth in children.
| Tags : airway, intubation, échographie
29/12/2014
Vidéolaryngoscopie: Un tournant ?
Techniques, Success, and Adverse Events of Emergency Department Adult Intubations
Brown CA et Al. Ann Emerg Med. 2014;-:1-9.
--------------------------------------------------------------------
Une certitude, l'emploi de vidéolaryngoscope simplifie l'abord trachéal pour les praticiens les moins expérimentés. Reste à démocratiser au plan économique ces dispositifs.
--------------------------------------------------------------------
Study objective: We describe the operators, techniques, success, and adverse event rates of adult emergency department (ED) intubation through multicenter prospective surveillance.
Methods: Eighteen EDs in the United States, Canada, and Australia recorded intubation data onto a Web-based data collection tool, with a greater than or equal to 90% reporting compliance requirement. We report proportions with binomial 95% confidence intervals (CIs) and regression, with year as the dependent variable, to model change over time.
Results: Of 18 participating centers, 5 were excluded for failing to meet compliance standards. From the remaining 13 centers, we report data on 17,583 emergency intubations of patients aged 15 years or older from 2002 to 2012. Indications were medical in 65% of patients and trauma in 31%. Rapid sequence intubation was the first method attempted in 85% of encounters.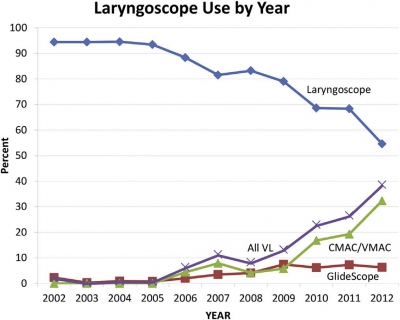 Emergency physicians managed 95% of intubations and most (79%) were physician trainees. Direct laryngoscopy was used in 84% of first attempts. Video laryngoscopy use increased from less than 1% in the first 3 years to 27% in the last 3 years (risk difference 27%; 95% CI 25% to 28%; mean odds ratio increase per year [ie, slope] 1.7; 95% CI 1.6 to 1.8). Etomidate was used in 91% and succinylcholine in 75% of rapid sequence intubations. Among rapid sequence intubations, rocuronium use increased from 8.2% in the first 3 years to 42% in the last 3 years (mean odds ratio increase per year 1.3; 95% CI 1.3 to 1.3). The first-attempt intubation success rate was 83% (95% CI 83% to 84%) and was higher in the last 3 years than in the first 3 (86% versus 80%; risk difference 6.2%; 95% CI 4.2% to 7.8%). The airway was successfully secured in 99.4% of encounters (95% CI 99.3% to 99.6%).
Emergency physicians managed 95% of intubations and most (79%) were physician trainees. Direct laryngoscopy was used in 84% of first attempts. Video laryngoscopy use increased from less than 1% in the first 3 years to 27% in the last 3 years (risk difference 27%; 95% CI 25% to 28%; mean odds ratio increase per year [ie, slope] 1.7; 95% CI 1.6 to 1.8). Etomidate was used in 91% and succinylcholine in 75% of rapid sequence intubations. Among rapid sequence intubations, rocuronium use increased from 8.2% in the first 3 years to 42% in the last 3 years (mean odds ratio increase per year 1.3; 95% CI 1.3 to 1.3). The first-attempt intubation success rate was 83% (95% CI 83% to 84%) and was higher in the last 3 years than in the first 3 (86% versus 80%; risk difference 6.2%; 95% CI 4.2% to 7.8%). The airway was successfully secured in 99.4% of encounters (95% CI 99.3% to 99.6%).
Conclusion: In the EDs we studied, emergency intubation has a high and increasing success rate. Both drug and device selection evolved significantly during the study period.
| Tags : airway, intubation
22/12/2014
Plus d'auscultation mais une Echo ?
Point of care ultrasound for orotracheal tube placement assessment in out-of hospital setting.
Zadel S et AL. Resuscitation. 2014 Nov 20;87C:1-6
-----------------------------------------------
A lire cet article, on comprend pourquoi l'engouement actuel pour l'échographie des voies aériennes. A coup sûr une technique à maîtriser en préhospitalier.
-----------------------------------------------
AIM OF THE STUDY:
The percentage of unrecognised orotracheal tube displacement in an out-of-hospital setting has been reported to be between 4.8% and 25%. The aim of our study was to assess the sensitivity and specificity of Point-of-Care-UltraSound (POCUS) for confirming the propertube position after an urgent orotracheal intubation in an out-of-hospital setting and the time needed for POCUS.
METHODS:
Our single-centred prospective study included all patients who needed out-of-hospital orotracheal intubation. After the intubation, bilateral chest auscultation and assessment of bilateral lung sliding and diaphragm excursion within POCUS were done. Spectrographic quantitative capnography was used as the reference standard to confirm a proper tube position.
RESULTS:
We enrolled 124 patients. For auscultation, sensitivity and negative predicted value were 100%, specificity was 90% and positive predicted value 30% (95% confidence interval).
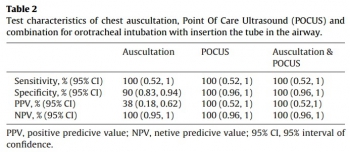
Sensitivity, specificity, positive predicted value, and negative predicted value for POCUS alone and for a combination of auscultation and POCUS were 100% (95% confidence interval). In three patients, we detected endobronchial tube displacement with auscultation and POCUS. Capnography failed to detect displacement in all three cases. The median time needed for POCUS was 30s.
CONCLUSION:
Results of our study support POCUS as an accurate and reliable method for confirming the proper orotracheal tube placement in trachea and it is feasible for out-of-hospital setting implementation. POCUS also seems to be time saving method but to make definitive conclusion more studies should be done.
| Tags : airway, intubation, échographie
15/12/2014
Anesthésie locale/régionale pour intubation
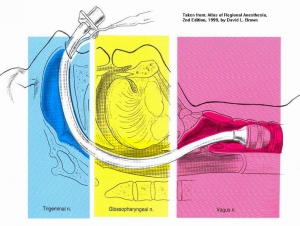
Regional and Topical Anesthesia for Endotracheal Intubation
En cas d'intubation difficile, il est important de préserver la ventilation spontanée. Il existe pour cela plusieurs techniques qui vous sont présentées en quelques images. Ces techniques permettent de faciliter l'intubation en évitant 3 réflexes du tronc particuliers: le gag reflexe (réflexe nauséeux) médié par le nerf glossopharyngé, le réflexe de fermeture glottique médié par les nerfs récurrents et laryngés supérieurs et le réflexe de toux médié par le vague.
1. L'anesthésie locale de glotte de proche en proche
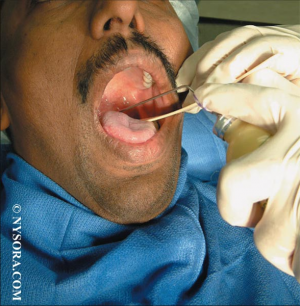
2. La nébulisation d'anesthésique local

3. Les blocs tronculaires
- a) Le bloc glossopharyngé
Anesthésie de l'oropharynx, de la portion postérieure de la langue et de la face antérieure de l'épiglotte

- b) Le bloc du nerf laryngé supérieur
Anesthésie de la base de la langue, de la surface postérieure de l'épiglotte, des replis aryépiglottiques et des aryténoïdes

-c) Le bloc transtrachéal des nerfs laryngés récurrents
anesthésie des cordes vocales et de la tachée

EN PRATIQUE solution 1 ou solution 2 ou association de 3b + 3c
Lire également:
Regional and Topical Anaesthesia of Upper Airways
Pani M et Al. Indian J Anaesth. Dec 2009; 53(6): 641–648.
14/12/2014
Sellick: Que disent les autres ?
La manoeuvre de Sellick
- Que disent les recommandations et RFE de nos sociétés savantes ?:
Cette manoeuvre est citée dans le document de la SFAR portant sur la "Prise en charge des voies aériennes en anesthésie adulte, à l'exception de l'intubation difficile". Il y est dit qu'elle "peut gêner l’exposition glottique au cours d’une laryngoscopie directe". Elle l'est également dans le document portant sur l'intubation difficile ("Dans le cadre de l’urgence, l’ISR avec manoeuvre de Sellick est la technique de référence"). Dans la recommandation portant sur l'abord trachéal pour la ventilation mécanique des malades de réanimation il est indiqué qu'une "séquence d'induction anesthésique rapide (préoxygénation, administration IV d'un agent anesthésique et d'un curare d'action rapide, compression cricoïdienne) permet d'obtenir de bonnes conditions d'intubation et une protection des voies aériennes". Cette manoeuve est également recommandée dans le document portant sur la sédation et analgésie en structure d’urgence : "La pression cricoïdienne (hors contre-indication) débutée dès la perte de conscience et maintenu jusqu’à la vérification de la position de la sonde endotrachéale. Cette pression cricoïdienne doit être levée en cas de vomissement"
- L'intérêt de la manoeuvre de Sellick n'est cependant plus le même qu'il y a quelques années (1, 2, 3).
- Que lit on dans les recommandations étrangères ?
1. Chez les Sud Africains
Is cricoid pressure necessary ? [Rapid sequence intubation. Emergenc medicine society of South Africa EM015 EM015B]
" We don’t know – the evidence supporting the use of cricoid pressure is fairly limited and there is more and more evidence emerging about the damaging effects of this manoeuvre. It is acceptable to omit the use of cricoid pressure in RSI. It is also acceptable to use cricoid pressure, as long as it is released if it interferes with bag-mask ventilation or laryngoscopy. .
........ The use of cricoid pressure during RSI in the EC is controversial. The consensus of expert opinion at this point in time is that cricoid pressure should be applied after the patient has lost consciousness after the administration of the induction agent and continuously maintained until the cuff has been inflated and the position of the ETT has been confirmed to be correct. This guideline is subject to the following provisos:
• Cricoid pressure should not be used if the assistant is not trained and experienced with the procedure. EMSSA Practice Guidelines provide advice on recommended practice for emergency centres, emergency personnel and emergency care activities. The information within these papers statements is advice only. EMSSA will not be held liable for clinical outcomes related to these Guidelines
• Cricoid pressure should immediately be released and not reapplied if: o There is any difficulty in bag-mask ventilation. o A supraglottic airway device is inserted. o There is any difficulty with laryngoscopy, including if external laryngeal manipulation is required (which cannot be performed while maintaining effective cricoid pressure). o The patient vomits.
• The doctor may also elect not to make use of cricoid pressure at all during the RSI."
2. En Europe du nord
Pre-hospital airway management: Scandinavian Society for Anaesthesiology and Intensive Care Medicine
Ils n'en parlent pas
3. Pour les suédois
Scandinavian clinical practice guidelines on general anaesthesia for emergency situations.
Jensenn AG et Al. Acta Anaesthesiol Scand 2010; 54: 922–950
"The use of cricoid pressure to reduce regurgitation is not based on scientific evidence. Therefore, its use cannot be recommended on the basis of scientific evidence. Anaesthesiologists can use the technique on individual judgement, but the anaesthesiologist must be ready to release the pressure if necessary. Cricoid pressure has been shown to limit the glottic view during laryngoscopy, and it should be releasedif such problems occur."
4. Pour les australiens
Emergency Airway Management in the Trauma Patient
"In conscious patients the cricoid cartilage is palpated between the thumb and middle finger, with the index finger above. The cricoid cartilage is located just below the prominent thyroid cartilage (Adam’s apple). As anaesthesia is induced the pressure is increased in a vertical plane onto the vertebral body of C5. The amount of pressure needs to approximate to 30 Newtons, comparable to the pressure that would feel uncomfortable if applied to the bridge of the nose. Removal of cricoid pressure should only follow securing of the airway and the request of the person performing intubation."
5. Pour les anglais
"Cricoid force: 10N awake 30N anaesthetise. If poor view: Reduce cricoid force. If Failed intubation: Maintain 30N cricoid force. Consider reducing cricoid force if ventilation difficult. If failed oxygenation: Reduce cricoid force during insertion of the LMA"
6. Pour les canadiens
"As cricoid pressure is likely to have potential benefits, its continued use seems prudent during rapid sequence intubation in the patient at high risk of aspiration (Strong recommendation for, level of evidence C). However, if difficulty is encountered with face mask ventilation or tracheal intubation, or if SGD insertion is needed, progressive or complete release of cricoid pressure is justified."
7. Chez les US
Drug-Assisted Intubation in the Prehospital Setting (NAEMSP Position Statement)
"While we recommend the application of cricoid pressure, we note that there are presently no data to support the effectiveness of this technique during prehospital airway management."
| Tags : airway
19/11/2014
Une bougie dans la sonde: c'est mieux.
Comparison of Intubation Performance by Emergency Medicine Residents Using Gum Elastic Bougie versus Standard Stylet in Simulated Easy and Difficult Intubation Scenarios
Walsh RM et All. Emerg Med Australas - ; 26 (5); 446-9
Study Objectives: We sought to evaluate the success rate and time to endotracheal intubation by emergency medicine residents with stylet reinforced endotracheal tube (ETT-S) versus intubation with a gum elastic bougie (GEB) in simulated easy and difficult airways on a cadaveric model.
Methods: The study was a prospective cross-over design using a single study cohort of 29 emergency medicine residents. A fresh frozen cadaver was used in either standard positioning to facilitate a Cormack Lehane Grade 1 laryngoscopy, or with a hard cervical collar applied a Cormack Lehane Grade 3 laryngoscopy. Each participant then intubated the cadaver in each setting (Grade 1 ETT-S, Grade 1 GEB, Grade 3 ETT-S, Grade 3 GEB). The primary end-point of our investigation was the time to intubation. Secondary endpoints were: success rate of intubation, mean ratings by study participants of perceived ease of intubation for each intubation technique in each simulated degree of difficulty, and overall preference of intubation technique in each simulated degree of difficulty. To assess the effect of intubation type (GEB vs ETT-S) and difficulty on time to successful intubation and perceived ease of intubation, repeated measures ANOVAs were conducted. To examine whether success of intubation differed across the GEB and ETT-S groups we used a McNemar’s test. To examine the effect of previous experience on time to intubation, we used a mixed model ANOVA incorporating intubation type and difficulty of intubation.
Results: Mean time to intubation in all scenarios ranged from 28.8 – 116.6 seconds. Year of residency training trended toward significance but was not significant when comparing post-graduate year to time to intubation (p¼ 0.07). Time to intubation was significantly different only when comparing Grade 3 ETTS to Grade 3 GEB (p¼ 0.006). Of the 116 intubations performed in this study, a total of 36 were failed attempts. There was no significant difference in success rate when comparing Grade 1 ETT-S to Grade 1 GEB nor Grade 3 ETT-S to Grade 3 GEB (p ¼ >0.05). Across all year groups, participants perceived the Grade 1 scenario to be easier than the Grade 3 scenario. At the conclusions of the study, 55% of participants preferred using the GEB in all settings. When broken down by scenario, 41% preferred the GEB in the Grade 1 scenario while 76% preferred the GEB in the Grade 3 scenario.
Conclusions: Time to intubation in a simulated grade 3 view was significantly longer in the GEB group versus the ETT-S group. Although the differences in success rates were not statistically significant, there was a trend toward more successful intubations with the GEB in the simulated grade 3 view. This is important because in the emergency department when difficult airways can be high stress and life threatening, although the GEB group took more time, the success rates were higher.
| Tags : intubation
11/11/2014
Videolaryngoscope en préhospitalier ? Pas si évident !
What is the role of video laryngoscopy in prehospital care ?
Voelckel WG et Al. Scand J Trauma Resusc Emerg Med. 2014; 22(Suppl 1): A6
Une réflexion qui exprime, malgré un apprentissage plus rapide et une meilleure vision, le manque actuel de données sur l'intérêt de la vidéolaryngoscopie préhospitalière. En effet meilleure vision ne signifie pas insertion plus facile du tube trachéal dans la trachée (lire ces argumentaires: 1, 2, 3, 4). Les auteurs lui prédisent cependant une place importante dans les années à venir.et en attendant:
APPRENEZ A INTUBER EN LARYNGOSCOPIE DIRECTE ET MAINTENEZ VOTRE SAVOIR FAIRE
| Tags : airway
11/10/2014
Suis je bien dans la trachée ?
Comment vérifier la position intratrachéale d'une sonde d'intubation ?
Le débat n'est pas nouveau (1). L'intérêt de l'intubation en condition de combat est d'ouvrir les voies aériennes, de prévenir le risque d'inhalation et de permettre l'application d'une ventilation adéquate. Son indication doit être bien mesurée car elle va ajouter une dimension de complexité pour un transport préhospitalier qui n'a rien à voir avec ce qui est rencontré en métropole.
Alors quelques réflexions ne sont pas inutiles car il faut éviter tant l'intubation oesophagienne que l'intubation sélective.
1. La visualisation de la sonde entre les cordes vocales est la base que ce soit au moment de la laryngoscopie initiale ou d'un contrôle après MAIS ce n'est pas suffisant, et pas forcément toujours possible.
2. La recherche d'une auscultation symétrique des 2 champs pulmonaires et d'un silence auscultatoire épigastrique doivent être fait MAIS ce n'est pas suffisant, et parfois difficile à obtenir.
3. L'expansion thoracique symétrique et la constatation de buée sur la sonde sont observées MAIS ce n'est pas suffisant.
4. Le recours à la mesure d'une SaO2 MAIS n'est pas du tout fait pour cela.
5. Utiliser une seringue ou un bulbe spécifique MAIS n'offre pas de certitude et c'est une techniQue peu diffusée en France
6. La CERTITUDE de l'intubation est donnée par la constatation de CO2 dans le gaz expiré à condition que soient respectés des critères quantitatifs et qualitatifs. Notamment les capnogrammes doivent être visualisés sur au moins 6 cycles ventilatoires durant lesquels l’absence de décroissance du signal confirme la bonne position de la sonde. (accéder à la conférence de consensus de la SFAR). Cette analyse qualitative est importante car le CO2 observé peut provenir d'air gastrique insufflé lors de ventilation manuelle voire d'anti-acides gastriques.
Mais dans notre contexte d'emploi la capnographie, telle que l'on la connait au bloc opératoire ou en SAUV, n'est pas le plus souvent disponible. Vous disposez de capteurs chimiques qui ne donnent qu'une estimation de la capnométrie. Certains disposent d'un capnomètre portable mais qui ne donne pas d'informations qualitatives. Enfin il existe des détecteurs oesophagiens dont la performance est bonne (2), sous réserve de conditions de stockage et d'emploi conforme notamment de température ambiante, mais qui ne permettent pas une surveillance continue et surtout si ils sont fiables pour confirmer la position intra-trachéale, ils le sont beaucoup moins pour la position intra-oeosophagienne.
7. Du nouveau arrive avec l'emploi de l'échographie pour valider la position intra-trachéale de la sonde d'intubation:
- soit par échographie cervicale (3, 4),
Kerforne T et al. Br. J. Anaesth. 2013;111:510-511
- soit par constatation de mouvements pleuraux bilatéraux (5)
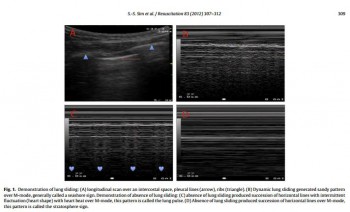
- ou encore d'une mobilité diaphragmatique lors de la ventilation (6)
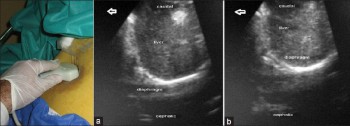
Int J Crit Illn Inj Sci. 2013 Apr;3(2):113-7
En contexte Militaire et en l'absence de capnographe, il faut, avant fixation de la sonde de vérification, dans le cadre la réalisation de mesures primaires de vérification de la bonne position de la sonde d'intubation ASSOCIER l'observation directe de la sonde franchissant les cordes vocales, l'expansion symétrique du thorax lors de la ventilation au ballon, la présence de buée dans la sonde, l'auscultation symétrique des deux champs pulmonaires et la présence de CO2 expiré sur le détecteur chimique. L'apport de l'échographie pourrait être d'être l'alternative à la radiographie pulmonaire pour la vérification secondaire de la bonne position de la sonde d'intubation.
Un débat qui porte sur la meilleure performance comparée à la capnographie et l'auscultation du repérage échographique est même déjà ouvert (7, 8, 9).
| Tags : airway
06/10/2014
Laryngoscopie directe: Toujours la référence en 1ère intention
Use of the Airtraq laryngoscope for emergency intubation in the prehospital setting: a randomized control trial.
Trimmel H et all. Crit Care Med 2011 Mar;39(3):489-93
__________________________________________
Une étude un peu ancienne mais qui a depuis été confirmée par d'autres (1, 2) et qui met bien en avant l'importance d'un apprentissage renforcé de la gestion des voies aériennes. Une méta-analyse plus récente le confirme (3).
__________________________________________
OBJECTIVES
The optical Airtraq laryngoscope (Prodol Meditec, Vizcaya, Spain) has been shown to have advantages when compared with direct laryngoscopy in difficult airway patients. Furthermore, it has been suggested that it is easy to use and handle even for inexperienced advanced life support providers. As such, we sought to assess whether the Airtraq may be a reliable alternative to conventional intubation when used in the prehospital setting.
DESIGN, SETTING, AND PATIENTS:
Prospective, randomized control trial in emergency patients requiring endotracheal intubation provided by anesthesiologists or emergency physicians responding with an emergency medical service helicopter or ground unit associated with the Department of Anesthesiology, General Hospital, Wiener Neustadt, Austria.
MEASUREMENTS AND MAIN RESULTS:
During the 18-month study period, 212 patients were enrolled. When the Airtraq was used as first-line airway device (n=106) vs. direct laryngoscopy (n=106), success rate was 47% vs. 99%, respectively (p<.001). Reasons for failed Airtraq intubation were related to the fiber-optic characteristic of this device (i.e., impaired sight due to blood and vomitus, n=11) or to assumed handling problems (i.e., cuff damage, tube misplacement, or inappropriate visualization of the glottis, n=24). In 54 of 56 patients where Airtraq intubation failed, direct laryngoscopy was successful on the first attempt; in the remaining two and in one additional case of failed direct laryngoscopy, the airway was finally secured employing the Fastrach laryngeal mask. There was no correlation between success rates and body mass index, age, indication for airway management, emergency medical service unit, or experience of the physicians.
CONCLUSIONS:
Based on these results, the use of the Airtraq laryngoscope as a primary airway device cannot be recommended in the prehospital setting without significant clinical experience obtained in the operation room. We conclude that the clinical learning process of the Airtraq laryngoscope is much longer than reported in the anesthesia literature.
| Tags : airway
20/09/2014
Intubation face à face: Du nouveau ?
Comparison of Sitting Face-to-Face Intubation (Two-Person Technique) with Standard Oral-tracheal Intubation in Novices: A Mannequin Study
J Emerg Med. 2012 Dec;43(6):1188-95

L'intubation face au patient n'est pas une nouveauté que ce soit en préhospitalier ou au bloc opératoire. Elle est cependant très peu fréquemment mise en oeuvre. Pourtant l'apparition des vidéolaryngoscopes, notamment l'airtraq, simplifie grandement cette pratique (vidéo ici). Certains s'interrogent sur son emploi plus large. Elle serait plus aisée que la laryngoscopie directe en décubitus dorsal. C'est ce que suggère ce document. Un grand recul est cependant nécessaire. Ce travail a été fait sur mannequin.
BACKGROUND:
Few studies have evaluated the impact of the upright position on the success of oral-tracheal intubation. Yet, for patients with airway difficulties (i.e, active intraoral bleeding or morbidly obese), the upright position may both benefit the patient and facilitate intubation.
OBJECTIVES:
We compared the success rates of subjects performing standard intubation to a modified version of the sitting face-to-face oral-tracheal intubation technique on a simulation model. We also reviewed the possible advantages and limitations of the sitting face-to-face intubationtechnique.
METHODS:
Volunteer medical and paramedical students were given instruction, then tested, performing in random order both standard oral-trachealand two-person sitting face-to-face oral-tracheal intubation on full-bodied mannequins. Observers reviewed video recordings, noting the number of successful intubations and the time to completion of each procedure at 15, 20, and 30 s.
RESULTS:
All of the sitting face-to-face intubations were successful, 53/53 (100%, 95% confidence interval [CI] 93-100%); whereas of the 53 subjects who performed standard intubation, 48 were successful (91%, 95% CI 80-96%). The difference between successful intubations using thestandard vs. sitting face-to-face technique was 9% (95% CI 1.3-9.4%, p=0.025). At times 15 and 20 s, medical student subjects who successfully performed both techniques were less successful at completing the procedure when performing the standard technique as compared to the sittingface-to-face technique (p=0.016). A post-procedural survey found that the majority of subjects preferred the sitting technique.
CONCLUSION:
Subjects were significantly more successful at performing and preferred the sitting face-to-face intubation when compared to standardintubation.
| Tags : airway
30/08/2014
Que font les israéliens en role 1
Role I trauma experience of the Israeli Defense Forces on the Syrian border
Benov A. et All. J Trauma Acute Care Surg. 2014 Sep;77(3 Suppl 2):S71-6
Une des particularités des actions conduites en role 1 par les équipes israéliennes est la maîtrise par leurs personnels des gestes de contrôle des voies aériennes, qu'il s'agisse de médecins ou de paramédic EMT-P. Cette publication l'illistre et confirme l'importance actuelle de ce savoir faire qui est donc ESSENTIEL pour une médicalisation réelle de l'avant.
---------------------------------------------------------------------------------------------------------------------
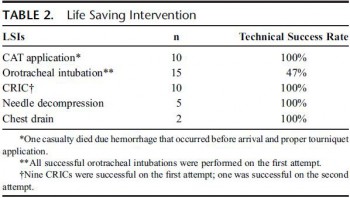
" Two-hundred fifty-eight casualties arrived at the border, 60 of whom were evaluated and returned to Syria. Of those, 15 received basic care and did not require any additional intervention, 39 experienced chronic conditions with no immediate need for medical attention, and 6 were dead on arrival. ......................Data from all echelons including prehospital information were available for 178 (90%) of the 198 patients, and this group constituted the study cohort. The extent of medical evacuation among the 178 casualtiesis as follows: 8 (4%) required only Role I care (debridement of wounds, removal of fragments, or death despite resuscitation attempts); 65 (36%) were evacuated to a Role 2+ facility and were later discharged; and 84 (47%) were evacuated to Role 3 civilian hospitals. ................................Eighteen patients underwent advanced airway procedures. Of 14 patients with a documented oxygen saturation of less than 90%, 5 improved following oxygen supplementation and did not require airway intervention. Of the 18 patients undergoing definitive airway management, head and face injury was present in two thirds (n = 11) of these, whereas a quarter (n = 4) had thoracic injury. The procedures were endotracheal intubation (ETI) (n = n = 15) and cricothyroidotomy (CRIC) (n = 10). Seven of eight casualties underwent CRI following failed initial attempt at ETI, and one patient was able to have mask ventilation following failed ETI. In three cases, CRIC was the first choice of airway management, two patients experiencing severe maxillofacial injury and one with severe laryngeal edema. There were no cases of preventable death due to airway obstruction and no complications from airway interventions. Forty-three casualties experienced thoracic injuries, five underwent chest decompression at a Role I facility by either needle decompression (n = 3) or insertion of a chest drain (n = 2).
| Tags : airway
03/07/2014
Dispositifs laryngés préhospitalier: Prudence !
Prehospital airway management using the laryngeal tube : An emergency department point of view.
Bernardht M. et Al Anaesthesist. 2014 Jul 2. [Epub ahead of print]
Il est proposé d'avoir recours à des dispositifs supra glottique pour la maîtrise de l'abord des voies aériennes en préhospitalier. Si ces dispositifs présentent des avantages avec notamment celui supposé d'une insertion plus simple que l'intubation ces derniers ont également des limites. AInsi l'engouement actuel doit il être tempéré par des inconvénients qui commencent à être décrits. C'est ce que rapporte l'article.
Parmi ceux ci, il y a les mauvais placement avec pour conséquence un défaut de ventilation du patient, un oedème obstructif de langue malgré des temps de pose court inférieur à 45 min et une situation d'intubation difficile, des problèmes d'étanchéité avec dans un cas une insufflation gastrique importante responsable d'un gêne à la ventilation contrôlée, un défaut de protection des voies aériennes avec inhalation du contenu gastrique.
Ce travail illustre donc que le recours aux dispositifs supraglottique ne doit pas être pensé comme une alternative à l'intubation qui permettrait à des opérateurs moins formés de pouvoir réaliser un geste de contrôle des voies aériennes. Il ne remet pas en cause l'intérêt de certains masques notamment les masques laryngés d'intubation qui on toute leur place dans la stratégie de gestion de l'intubation difficile. Enfin en condition de combat on rappelle que les 3 techniques dont la maîtrise doit être parfaite sont la ventilation manuelle, l'intubation oro-trachéale avec ISR et la coniotomie. Ceci est également le positionnement de l'armée israélienne. On retrouve là, comme avec l'exsufflation des pneumothorax avec des aiguilles de 8 cm en lieu et place des cathéters courants, outre la prudence nécessaire à avoir face à des avantages apparents sans analyses des inconvénients associés.
BACKGROUND:
Competence in airway management and maintenance of oxygenation and ventilation represent fundamental skills in emergency medicine. The successful use of laryngeal tubes (LT, LT-D, LTS II) to secure the airway in the prehospital setting has been published in the past. However, some complications can be associated with the use of a laryngeal tube.
METHODS:
In a nonconsecutive case series, problems and complications associated with the use of the laryngeal tube in prehospital emergency medicine as seen by independent observers in the emergency room are presented.
RESULTS:
Various problems and possible complications associated with the use of a laryngeal tube in eight case reports are reported: incorrect placement of the laryngeal tube in the trachea, displacement and/or incorrect placement of the laryngeal tube in the pharynx, tongue and pharyngeal swelling with subsequently difficult laryngoscopy, and inadequate ventilation due to unrecognized airway obstruction and tension pneumothorax.
CONCLUSION:
Although the laryngeal tube is considered to be an effective, safe, and rapidly appropriable supraglottic airway device, it is also associated with adverse effects. In order to prevent tongue swelling, after initial prehospital or in-hospital placement of laryngeal tube and cuff inflation, it is important to adjust and monitor the cuff pressure.
| Tags : airway
13/06/2014
Airway Cam Portal
![]()
Cliquer sur l'image pour accéder au site
| Tags : airway
05/06/2014
Réflexions US sur l'accès aux voies aériennes
Advances in prehospital airway management
Jacobs PE et all. Int J Crit Illn Inj Sci. 2014 Jan-Mar; 4(1): 57–64.
Prehospital airway management is a key component of emergency responders and remains an important task of Emergency Medical Service (EMS) systems worldwide. The most advanced airway management techniques involving placement of oropharyngeal airways such as the Laryngeal Mask Airway or endotracheal tube. Endotracheal tube placement success is a common measure of out-of-hospital airway management quality. Regional variation in regard to training, education, and procedural exposure may be the major contributor to the findings in success and patient outcome. In studies demonstrating poor outcomes related to prehospital-attempted endotracheal intubation (ETI), both training and skill level of the provider are usually often low. Research supports a relationship between the number of intubation experiences and ETI success. National standards for certification of emergency medicine provider are in general too low to guarantee good success rate in emergency airway management by paramedics and physicians. Some paramedic training programs require more intense airway training above the national standard and some EMS systems in Europe staff their system with anesthesia providers instead. ETI remains the cornerstone of definitive prehospital airway management, However, ETI is not without risk and outcomes data remains controversial. Many systems may benefit from more input and guidance by the anesthesia department, which have higher volumes of airway management procedures and extensive training and experience not just with training of airway management but also with different airway management techniques and adjuncts.
| Tags : airway, intubation
01/06/2014
Pression cricoïdienne: Plus recommandé
La manoeuvre de Sellick, si classique, n'est plus recommandée ou du moins il est considéré qu'elle ne dispose plus d'assez d'arguments pour en faire une manoeuvre obligatoire.
Cliquez sur l'image qui suit pour un point actualisé
Les recommandations de l'Eastern Association for the Surgery of Trauma
| Tags : intubation
23/05/2014
Manoeuvre de Sellick: Questions/Réponses
Cricoid Pressure in Emergency Department Rapid Sequence Tracheal Intubations: A Risk-Benefit Analysis
Ellis DY et Al. An Emerg Med. 2007 Dec;50(6):653-65
La manœuvre de Sellick est une technique de compression du cartilage cricoïde, décrite en 1961 par Sellick BA. Lors de la réalisation d'une intubation trachéale, elle est utilisée pour prévenir le risque de régurgitation du contenu gastrique et œsophagien vers le pharynx et son inhalation bronchique et alvéolaire lors de l'induction anesthésique qui entraîne une dépression des réflexes de protection des voies aériennes, chez un patient dont l’estomac est plein.
Elle consiste à appuyer fermement sur le cartilage cricoïde qui va alors comprimer l'extrémité supérieure de l'œsophage dont les parois sont souples, contre le corps vertébral de la vertèbre cervicale sous-jacente, rigide. L'intensité de la force à exercer doit être d'environ 20 newtons (N) si le patient est conscient et de 30 N s'il est inconscient2. Cette force est suffisante pour prévenir la régurgitation (inefficace si inférieure à 10 N), n'entraîne pas de sensation nauséeuses susceptibles d'augmenter l'inhalation du contenu gastrique et met à l'abri d'une rupture œsophagienne.
Le taux d'efficacité de la manœuvre de Sellick n'est pas bien établi, techniquement simple, elle est pourtant souvent mal réalisée.
-----------------------------------------------------------------------
Cricoid pressure is considered an integral part of patient safety in rapid sequence tracheal intubation and emergency airway management. Cricoid pressure is applied to prevent the regurgitation of gastric contents into the pharynx and subsequent aspiration into the pulmonary tree. This review analyzes the published evidence supporting cricoid pressure, along with potential problems, including increased difficulty with tracheal intubation and ventilation. According to the evidence available, the universal and continuous application of cricoid pressure during emergency airway management is questioned. An awareness of the benefits and potential problems with technique allows the practitioner to better judge when cricoid pressure should be used and instances in which it should be removed.
-----------------------------------------------------------------------
Le travail présenté répond à un certain nombre d'interrogations et précise pourquoi la réalisation de cette manoeuvre est remise en question.
| Tags : airway
08/04/2014
Coniotomie au Combat: Simuler pour retenir le savoir
Effect of Simulation Training on Compliance with Difficult Airway Management Algorithms, Technical Ability, and Skills Retention for Emergency Cricothyrotomy
Vincent H. et Al. Anesthesiology 2014; 120:999-1008
background:
The effectiveness of simulation is rarely evaluated. The aim of this study was to assess the impact of a short training course on the ability of anesthesiology residents to comply with current difficult airway management guidelines.
METHODS:
Twenty-seven third-year anesthesiology residents were assessed on a simulator in a "can't intubate, can't ventilate" scenario before the training (the pretest) and then randomly 3, 6, or 12 months after training (the posttest). The scenario was built so that the resident was prompted to perform a cricothyrotomy. Compliance with airway management guidelines and the cricothyrotomy's duration and technical quality were assessed as a checklist score [0 to 10] and a global rating scale [7 to 35].
RESULTS:
After training, all 27 residents (100%) complied with the airway management guidelines, compared with 17 (63%) in the pretest (P < 0.005). In the pretest and the 3-, 6-, and 12-month posttests, the median [range] duration of cricothyrotomy was respectively 117 s [70 to 184], 69 s [43 to 97], 52 s [43 to 76], and 62 s [43 to 74] (P < 0.0001 vs. in the pretest), the median [range] checklist score was 3 [0 to 7], 10 [8 to 10], 9 [6 to 10], and 9 [4 to 10] (P < 0.0001 vs. in the pretest) and the median [range] global rating scale was 12 [7 to 22], 30 [20 to 35], 33 [23 to 35], and 31 [18 to 33] (P < 0.0001 vs. in the pretest). There were no significant differences between performance levels achieved in the 3-, 6-, and 12-month posttests.

CONCLUSION: The training session significantly improved the residents' compliance with guidelines and their performance of cricothyrotomy.
| Tags : airway, intubation
07/04/2014
Airway en préhospitalier US: Plus tube que dispositif glottique
An update on out-of-hospital airway management practices in the United States
Diggs LA. et Al. Resuscitation. 2014 Mar 15. pii: S0300-9572
______________________________________________________
Ce document fait le point sur la pratique préhospitalière US. Cette dernière est faite avant tout d'intubation et la prudence est de mise concernant les performances réelles des dispositifs supra-glottiques avec lesquels (excepté le tube de king) les résultats sont moins bons.
______________________________________________________
OBJECTIVE: We characterized out-of-hospital airway management interventions, outcomes, and complications using the 2012 NEMSIS Public-Release Research Data Set containing almost 20 million Emergency Medical Services activations from 40 states and two territories. We compared the outcomes with a previous study that used 2008 NEMSIS data containing 16 states with 4 million EMS activations.
METHODS:
Patients who received airway management interventions including endotracheal intubation (ETI), alternate airways (Combitube, Laryngeal Mask Airway (LMA), King LT, Esophageal-Obturator Airway (EOA)), and cricothyroidotomy (needle and surgical) were identified. Using descriptive statistics, airway management success and complications were examined in the full cohort and key subsets including cardiac arrest, non-arrest medical, non-arrest injury, children<10 years, children 10-19 years, rapid sequence intubation (RSI), population setting, US census region, and US census division.
RESULTS:
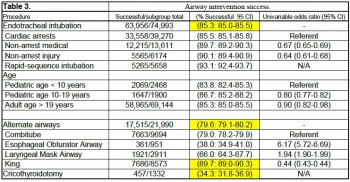
Among 19,831,189 EMS activations, there were 74,993 ETIs, 21,990 alternate airways, and 1332 cricothyroidotomies. ETI success rates were: overall 63,956/74,993 (85.3%; 95% CI: 85.0-85.5), cardiac arrest 33,558/39,270 (85.5%), non-arrest medical 12,215/13,611 (89.7%), non-arrest injury (90.1%), children<10 years 2069/2468 (83.8%), children 10-19 years 1647/1900 (86.7%), adults>19 years 58,965/69,144 (85.3%), and rapid sequence intubation 5265/5658 (93.1%). Major complications included bleeding 677 (4.4 per 1000 interventions), vomiting 1221 (8 per 1000 interventions), esophageal intubation immediately detected 874 (5.7 per 1000 interventions), and esophageal intubations other 219 (1.4 per 1000 interventions).
CONCLUSIONS:
Paramedics provide life-saving emergency medical care to patients in the out-of-hospital setting. Only selected emergency medical procedures have proved to be safe and effective. The safety and efficacy profile of ETI has been challenged in the last ten years. Intubation has been the standard of care in the United States for more than thirty years and is regarded as one of the most important EMS procedures. In this study, we retrospectively examined the largest aggregate of EMS data currently available and observed low out-of-hospital ETI success rates.
ETI is a complex procedure requiring skilled choreography and numerous critical decisions and actions. In the absence of qualified personnel, or if ETI proves problematic, alternate airways are commonly employed. As more EMS systems embrace alternate airway devices in lieu of ETI, it is important to have a clear appreciation of the true success rates of airway procedures using these devices across a variety of patient characteristics and clinical settings. This study examined the most commonly used alternate airway devices including the Combitube, Esophageal Obturator Airway, Laryngeal Mask Airway, King Laryngeal Tube, and cricothyroidotomy and observed very low alternate airway success rates in the largest population sample to date. Alternate airway success rates were substantially lower than ETI success rates except for the King LT.
| Tags : airway, intubation
01/04/2014
Bougie d'intubation: Pas toutes égales
Bougie-related airway trauma: dangers of the hold-up sign
Marson BA et Al. Anaesthesia 2014, 69, 219–223
Le bon positionnement d'un mandrin d'intubation est confirmé parles sensations de ressaut quand l'extrémité de ce dernier franchit les anneaux trachéaux et par le blocage de ce dernier dans l'arbre bronchique. Ce dernier signe est appelé "the hold up sign" par les anglo-saxons. Ce blocage confirme que le mandrin n'est pas intra-oesophagien auquel cas il n'existerait pas. Cette publication attire l'attention sur le danger potentiel de traumatisme trachéal.
----------------------------------------------------------------------------
The bougie is a popular tool in difficult intubations. The hold-up sign is used to confirm tracheal placement of a bougie. This study aimed to establish the potential for airway trauma when using this sign with an Eschmann reusable bougie or a Frova single-use bougie. Airways were simulated using a manikin (hold-up force) and porcine lung model (airway perforation force). Mean (SD) hold-up force (for airway lengths over the range 25–45 cm) of 1.0 (0.4) and 5.2 (1.1) N were recorded with the Eschmann and Frova bougies, respectively (p < 0.001). The mean (SD) force required to produce airway perforation was 0.9 (0.2) N with the Eschmann bougie and 1.1 (0.3) N with the Frova bougie (p = 0.11). It is possible to apply a force at least five times greater than the force required to produce significant trauma with a Frova single-use bougie. We recommend that the hold-up sign should no longer be used with single-use bougies. Clinicians should be cautious when eliciting this sign using the Eschmann re-usable bougie.
--------------------------------------------------------------------------------------------------------------
Il existe d'autres bougies que celle d'eschmann et de Frova comme l'Introes pocket bougie ou la traffic light bougie. Cette dernière apparaît très intéressante car permettant de limiter la longueur de mandrin inséré dans la trachée et partant le risque de perforation trachéale.
| Tags : intubation
29/01/2014
Trauma ballistique de la face: 1/3 nécessitent un airway sécurisé
Gunshot wounds and blast injuries to the face are associated with significant morbidity and mortality: Results of an 11-year multi-institutional study of 720 patients
Shackford et All. J Trauma Acute Care Surg. 2014;76: 347-352
BACKGROUND:
Gunshot wounds and blast injuries to the face (GSWBIFs) produce complex wounds requiring management by multiple surgical specialties. Previous work is limited to single institution reports with little information on processes of care or outcome. We sought to determine those factors associated with hospital complications and mortality.
METHODS:
We performed an 11-year multicenter retrospective cohort analysis of patients sustaining GSWBIF. The face, defined as the area anterior to the external auditory meatuses from the top of the forehead to the chin, was categorized into three zones: I, the chin to the base of the nose; II, the base of the nose to the eyebrows; III, above the brows. We analyzed the effect of multiple factors on outcome.
RESULTS:
From January 1, 2000, to December 31, 2010, we treated 720 patients with GSWBIF (539 males, 75%), with a median age of 29 years. The wounding agent was handgun in 41%, explosive (shotgun and blast) in 20%, rifle in 6%, and unknown in 33%. Prehospital or resuscitative phase airway was required in 236 patients (33%). Definitive care was rendered by multiple specialties in 271 patients (38%). Overall, 185 patients died (26%), 146 (79%) within 48 hours. Of the 481 patients hospitalized greater than 48 hours, 184 had at least one complication (38%). Factors significantly associated with any of a total of 207 complications were total number of operations (p < 0.001), Revised Trauma Score (RTS, p < 0.001), and head Abbreviated Injury Scale (AIS) score (p < 0.05). Factors significantly associated with mortality were RTS (p < 0.001), head AIS score (p < 0.001), total number of operations (p < 0.001), and age (p < 0.05). An injury located in Zone III was independently associated with mortality (p < 0.001).
CONCLUSION:
GSWBIFs have high mortality and are associated with significant morbidity. The multispecialty involvement required for definitive care necessitates triage to a trauma center and underscores the need for an organized approach and the development of effective guidelines.
| Tags : airway