11/11/2016
15 ans d'emploi du tourniquet: Que dire ?
Battlefield Tourniquets: Lessons Learned in Moving Current Care Toward Best Care in an Army Medical Department at War
Kragh JF Jr et Al. US Army Med Dep J. 2016 Apr-Sep;(2-16):29-36.
------------------------------
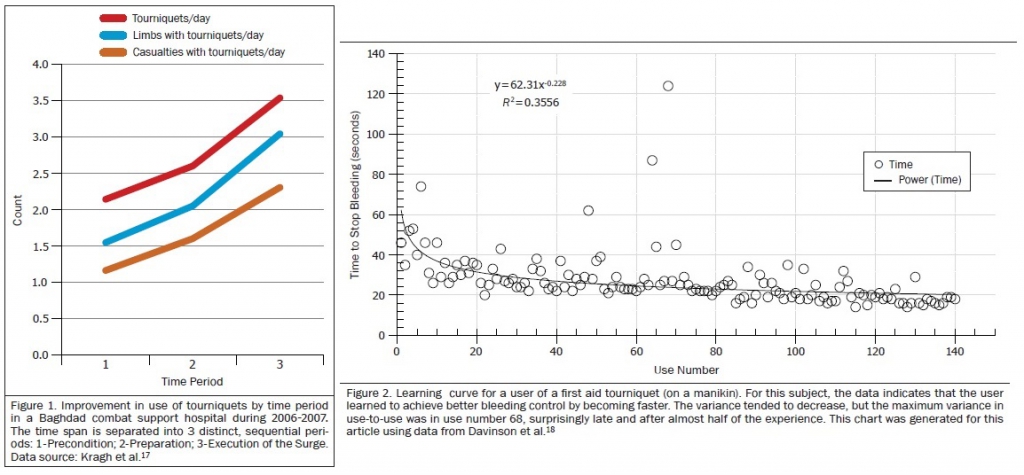
Un point d'étape qui insiste sans surprise sur l'apport d'une pose précoce d'un garrot. Précoce mais aussi rapide: 25 secondes sont nécessaires aux plus entraînés mais c'est 20 secondes de trop. Plus on s'entraîne et plus vite ET mieux on pose ce garrot.
------------------------------
Bleeding prevention and control by tourniquet use by out-of-hospital caregivers is a major breakthrough in military medicine of current wars. The present review documents developments in tourniquet practices since 2001 among the US military services for aid in improving doctrine, policy, and especially care in wars to come. Tourniquets are an adjunct for resuscitation in self-care and buddy aid and today are issued to all military service persons who deploy into a combat zone. In the US Army, virtually every Soldier is trained in first aid tourniquet use; since 2009 they are instructed early and often to use them early and often. Despite substantial knowledge gains among the services in tourniquet use and resulting improvements in casualty survival, current evidence shows persistent diffi culties in achieving best care with tourniquet use for individual trauma patients. Nevertheless, contemporary tourniquet use incorporates key lessons learned over the last 14 years of war that include: (1) tourniquet use reliably stops bleeding from limb wounds and prevents mortality in prehospital settings; and (2) brief tourniquet use appears to be safe. These 2 lessons have become so evident that civilian emergency medical systems have begun using them, albeit unevenly. Collection and interpretation of data of casualties with tourniquet use have showed that such intervention has lifesaving benefit through 2 mechanisms: control of both ongoing hemorrhage and shock severity. The next generation of interventions in bleeding control involves developing the skill sets, education, and standards of tourniquet users which may improve hemorrhage control in wars to come
| Tags : tourniquet
24/09/2016
Tourniquet: Entretien 3/mois mieux qu'1/mois
Does practice make perfect? Prospectively comparing effects of 2 amounts of practice on tourniquet use performance
---------------------------------------------
L'entretien des compétences et en particulier des gestes apparaît fondamentale et nécessite un suivi chiffré pour garantir un niveau suffisant d'expertise pour une projection opérationnelle. Ceci est parfaitement mis en avant dans le travail de schaeur et Al. (1) qui porte sur des gestes de réanimation préhospitalière. Le document proposé à votre lecture porte sur un geste essentiel: La pose du garrot. Une pratique plus régulière limite le désapprentissage.
---------------------------------------------
Although a lifesaving skill, currently, there is no consensus for the required amount of practice in tourniquet use. We compared the effect of 2 amounts of practice on performance of tourniquet use by nonmedical personnel.
METHODS:
Israeli military recruits without previous medical training underwent their standard tactical first aid course, and their initial performance in use of the Combat Application Tourniquet (CAT; Composite Resources, Rock Hill, SC) was assessed. The educational intervention was to allocate the participants into a monthly tourniquet practice program: either a single-application practice (SAP) group or a triple-application practice (TAP) group. Each group practiced according to its program. After 3 months, the participants' tourniquet use performance was reassessed. Assessments were conducted using the HapMed Leg Tourniquet Trainer (CHI Systems, Fort Washington, PA), a mannequin which measures time and pressure.
RESULTS:
A total of 151 participants dropped out, leaving 87 in the TAP group and 69 in the SAP group. On initial assessment, the TAP group and the SAP group performed similarly. Both groups improved their performance from the initial to the final assessment. The TAP group improved more than the SAP group in mean application time (faster by 18 vs 8 seconds, respectively; P = .023) and in reducing the proportion of participants who were unable to apply any pressure to the mannequin (less by 18% vs 8%, respectively; P = .009).
CONCLUSION:
Three applications per monthly practice session were superior to one. This is the first prospective validation of a tourniquet practice program based on objective measurements.
| Tags : tourniquet
04/09/2016
Garrot: Mais l'occlusion dans le temps ?
Different Width and Tightening System: Emergency Tourniquets on Distal Limb Segments
BACKGROUND:
Tourniquets are used on distal limb segments. We examined calf and forearm use of four thigh-effective, commercial tourniquetswith different widths and tightening systems: 3.8 cm windlass Combat Application Tourniquet® (CAT, combattourrniquet.com) and Special Operations Forces® Tactical Tourniquet-Wide (SOFTTW, www.tacmedsolutions.com), 3.8 cm ratchet Ratcheting Medical Tourniquet - Pediatric (RMT-P, www.ratchetingbuckles. com), and 10.4 cm elastic Stretch-Wrap-And-Tuck Tourniquet® (SWATT, www.swattourniquet.com).
METHODS:
From Doppler-indicated occlusion, windlass completion was the next securing opportunity; ratchet completion was one additional tooth advance; elastic completion was end tucked under a wrap.
RESULTS:
All applications on the 16 recipients achieved occlusion. Circumferences were calf 38.1±2.5 cm and forearm 25.1±3.0 cm (p<.0001, t-test, mean±SD). Pressures at Occlusion, Completion, and 120-seconds after Completion differed within each design (p<.05, one-way ANOVA; calf: CAT 382±100, 510±108, 424±92 mmHg; SOFTT-W 381±81, 457±103, 407±88 mmHg; RMT-P 295±35, 350±38, 301±30 mmHg; SWATT 212±46, 294±59, 287±57 mmHg; forearm: CAT 301±100, 352±112, 310±98 mmHg; SOFTT-W 321±70, 397±102, 346±91 mmHg; RMT-P 237±48, 284±60, 256±51 mmHg; SWATT 181±34, 308±70, 302±70 mmHg). Comparing designs, pressures at each event differed (p<.05, one-way ANOVA), and the elastic design had the least pressure decrease over time (p<.05, one-way ANOVA). Occlusion losses differed among designs on the calf (p<.05, χ²; calf: CAT 1, SOFTT-W 5, RMT-P 1, SWATT 0; forearm: CAT 0, SOFTT-W 1, RMT-P 2, SWATT 0).
CONCLUSIONS:
All four designs can be effective on distal limb segments, the SWATT doing so with the lowest pressures and least pressure losses over time. The pressure change from Occlusion to Completion varies by tourniquet tightening system and can involve a pressure decrease with the windlass tightening systems. Pressure losses occur in as little as 120 seconds following Completion and so can loss of Occlusion. This is especially true for nonelastic strap tourniquet designs.
| Tags : tourniquet
2 garrots: Côte à côte SVP, mais attention
Pressures Under 3.8cm, 5.1cm, and Side-by-Side 3.8cm-Wide Tourniquets
-----------------------------
Plus un garrot est large et plus efficace il est. parmi les garrots en dotation le Garrot Delfi est le plus performant en terme d'occlusion. Néanmoins son emploi en première intention et hors un vecteur d'évacuation est difficilement envisageable. Aussi l'association de deux garrots apparaît elle très pertinente surtout si ces derniers sont posés côte à côte. Ce n'est pas pour autant une sécurité car en permettant l'obtention d'une pression d'occlusion plus basse, cette méthode expose à une occlusion insuffisante . Cette publication a par ailleurs comme intérêt de montrer que la pression d'occlusion baisse avec le temps et ce dès les premières minutes. Il est fondamental d'apprécier TRES régulièrement l'efficacité du garrot. Donc plutôt un garrot large d'emblée mais si l'on doit compléter poser le second à côté du premier. A noter que le garrot utilisé n'est pas en dotation dans l'armées US mais qu'il s'agit d'un des meilleurs garrots de dernière génération.
-----------------------------
BACKGROUND:
Applications of wider tourniquet are expected to occlude arterial flow at lower pressures. We examined pressures under 3.8cm-wide, 5.1cm-wide, and side-by-side-3.8cm-wide nonelastic strap-based tourniquets.
METHODS:
Ratcheting Medical Tourniquets (RMT) were applied mid-thigh and mid-arm for 120 seconds with Doppler-indicated occlusion. The RMTs were a Single Tactical RMT (3.8cm-wide), a Wide RMT (5.1cm-wide), and Paired Tactical RMTs (7.6cm-total width). Tightening completion was measured at one-tooth advance past arterial occlusion, and paired applications involved alternating tourniquet tightening.
RESULTS:
All 96 applications on the 16 recipients reached occlusion. Paired tourniquets had the lowest occlusion pressures (ρ < .05). All pressures are given as median mmHg, minimum-maximum mmHg. Thigh application occlusion pressures were Single 256, 219-299; Wide 259, 203-287; Distal of Pair 222, 183-256; and Proximal of Pair 184, 160-236. Arm application occlusion pressures were Single 230, 189-294; Wide 212, 161-258; Distal of Pair 204, 193-254, and Proximal of Pair 168, 148-227. Pressure increases with the final tooth advance were greater for the 2 teeth/cm Wide than for the 2.5 teeth/cm Tacticals (ρ < .05). Thigh final tooth advance pressure increases were Single 40, 33-49; Wide 51, 37-65; Distal of Pair 13, 1-35; and Proximal of Pair 15, 0-30. Arm final tooth advance pressure increases were Single 49, 41-71; Wide 63, 48-77; Distal of Pair 3, 0-14; and Proximal of Pair 23, 2-35. Pressure decreases occurred under all tourniquets over 120 seconds. Thigh pressure decreases were Single 41, 32-75; Wide 43, 28-62; Distal of Pair 25, 16-37; and Proximal of Pair 22, 15-37. Arm pressure decreases were Single 28, 21-43; Wide 26, 16-36; Distal of Pair 16, 12-35; and Proximal of Pair 12, 5-24. Occlusion losses before 120 seconds occurred predominantly on the thigh and with paired applications (ρ < .05). Occlusion losses occurred in six Paired thigh applications, two Single thigh applications, and one Paired arm application.
CONCLUSIONS:
Side-by-side tourniquets achieve occlusion at lower pressures than single tourniquets. Additionally, pressure decreases undertourniquets over time; so all tourniquet applications require reassessments for continued effectiveness.
| Tags : tourniquet
22/12/2015
Tourniquet: Contrefaçons=Danger
Le regain d'intérêt pour la mise en place de garrot en cas d'hémorragie massive des membres ne doit pas faire oublier deux choses: Avoir appris correctement et utiliser un matériel adhoc.
Concernant ce dernier point apparaissent sur le marché nombre de garrots qui soit n'ont pas été validés soit sont des contrefaçons de ce dernier, soit des garrots proposés dans le cadre d'activité de type Softball.
Plutôt que d'utiliser un garrot de piêtre qualité, il vaut probablement mieux avoir recours à un garrot artisanal dont l'efficacité n'est pas remise en cause sous réserve d'une technique de pose maîtrisée.
On rappelle que les 3 seuls garrots validés par l'armée américaine sont le CAT, le SOFTT et le Delfi EMT. Les SEULS garrots en service dans l'armée française sont le SOFTT et le Delfi EMT. Ces garrots sont produits par des industriels au terme de travaux de recherche et de démarche d'évolution et de politique qualité aboutis, toutes démarches absentes chez les copieurs et les contrefacteurs.
Tous les autres garrots n'ont pas suivis les mêmes process de développement, ce qui ne permet pas de garantir ni leur efficacité dans le temps, ni leur fiabilité.
Un exemple de copie du SOFTT est ici présenté

Un point d'alerte majeur aux USA
| Tags : tourniquet
18/07/2015
Tourniquet et chaleur extrême ?
Laboratory testing of emergency tourniquets exposed to prolonged heat
Davidson JP et Al. J Spec Oper Med. 2015 Spring;15(1):34-8.
----------------------------------------------------------
Il a été démontré que la fiabilité mécanique des tourniquets pouvait être altérée si ces derniers n'étaient pas protégés (1,2,3). Le travail présenté porte sur l'effet de l'exposition prolongée à de hautes températures sur l'efficacité des garrots. Apparemment il n'y aurait pas d'effet propre.
----------------------------------------------------------
BACKGROUND:
Environmental exposure of tourniquets has been associated with component damage rates, but the specific type of environmental exposure, such as heat, is unknown. Emergency-tourniquet damage has been associated with malfunction and loss of hemorrhage control, which may risk loss of life during first aid. The purposes of the study are to determine the damage rate of tourniquets exposed to heat and to compare the rate to that of controls.
METHODS:
Three tourniquet models (Combat Application Tourniquet®; SOF® Tactical Tourniquet; Ratcheting Medical Tourniquet®) were tested using a manikin (HapMed Leg Tourniquet Trainer; www.chisystems.com) that simulates extremity hemorrhage. The study group of 15 tourniquets (five devices per model, three models) was exposed to heat (oven at 54.4° C [130° F] for 91 days), and 15 tourniquets similarly constituted the control group (unexposed to heat). Damage, hemorrhage control, distal pulse stoppage, time to effectiveness, pressure (mmHg), and blood loss volumes were measured.
RESULTS:
Three tourniquets in both groups had damage not associated with heat exposure (p = 1). Heat exposure was not associated with change in effectiveness rates (p = .32); this lack of association applied to both hemorrhage control and pulse stoppage. When adjusted for the effects of user and model, the comparisons of time to effectiveness and total blood loss were statistically significant (p < .0001), but the comparison of pressure was not (p = .0613).
CONCLUSION:
Heat exposure was not associated with tourniquet damage, inability to gain hemorrhage control, or inability to stop the distal pulse.
| Tags : tourniquet
17/07/2015
Tourniquet: Une histoire de pression pas si simple
Tourniquets and Occlusion: The Pressure of Design
Wall PL et Al. Mil Med. 2013 May;178(5):578-87
-----------------------------------------------
Un travail très intéressant qui exprime bien que l'efficacité d'un garrot nécessite un ensemble de gestes parfaitement réalisés, notamment un serrage suffisant qui doit être vérifié après la pose. Il existe en effet avec les garrots de type tourniquet ou pneumatique une chute plus ou moins importante de la pression d'occlusion donc de perte d'occlusion, ce d'autant qu'un relâchement musculaire peut apparaître réduisant d'autant plus cette pression d'occlusion. Les garrots élastiques n'aurait pas cet inconvénient.
-----------------------------------------------
Abstracts: Nerve injuries result from tourniquet pressure. The objective was to determine arterial occlusion and completion pressures with the 3.8-cm-wide windlass Combat Application Tourniquet (CAT) and the 10.4-cm-wide Stretch, Wrap, and Tuck Tourniquet (SWAT-T).
Methods: Sixteen volunteers self-applied and had tourniquets applied to their thighs and arms (CAT and SWAT-T, random order, then blood pressure cuffs).
Results: Occlusion (Doppler signal elimination) pressures were higher than predicted ( p < 0.0001), highest with the CAT ( p < 0.0001), and often lower than completion pressures (completion median, range: CAT 360, 147–745 mm Hg; SWAT-T 290, 136–449 mm Hg; cuff 184, 108–281 mm Hg). Three CAT thigh and 9 CAT arm completion pressures were >500 mm Hg. Pressure decreases and occlusion losses occurred over 1 minute (pressure decrease: CAT 44 ± 33 mm Hg; SWAT-T 6 ± 8 mm Hg; cuff 14 ± 19 mm Hg; p < 0.0001; loss/initially occluded: CAT 17 of 61, SWAT-T 5 of 61, cuff 40 of 64, p < 0.01). CAT pressures before turn did not have a clear relationship with turns to occlusion.
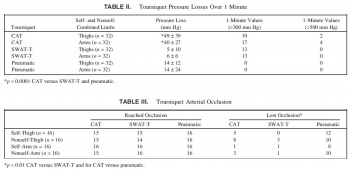 Conclusions: Limb circumference/ tourniquet width occlusion pressure predictions are not good substitutes for measurements. The wider SWAT-T has lower occlusion and completion pressures than the CAT. Decreases in muscle tension lead to decreases in tourniquet pressure, especially with the nonelastic CAT, which can lead to occlusion loss.
Conclusions: Limb circumference/ tourniquet width occlusion pressure predictions are not good substitutes for measurements. The wider SWAT-T has lower occlusion and completion pressures than the CAT. Decreases in muscle tension lead to decreases in tourniquet pressure, especially with the nonelastic CAT, which can lead to occlusion loss.
| Tags : tourniquet
21/03/2015
Tourniquet: Efficace, uniquement si serré fort
Forward Assessment of 79 Prehospital Battlefield Tourniquet Use in the Current War
King DR et Al. J Spec Oper Med. 2012 Winter;12(4):33-8.
----------------------------------------------------------------------
La pose libérale d'un garrot est présentée comme étant un facteur essentiel de survie des blessés des membres. Encore faut il que ces derniers soient posés de manière correcte. Le document présenté laisse planer un gros doute. En effet il met en évidence qu'un garrot est mis en place 3 fois sur 4 alors qu'il n'y a pas de lésion vasculaire notable et que la plupart des garrots posés ne sont pas suffisamment serrés et sont en fait des garrots veineux. Pire seuls 1/3 des blessés ayant des lésions artérielles se voient appliquer un garrot artériel. C'est dire qu'une attention particulière doit être portée sur l'abolition du pouls artériel distal. Il s'agit là d'un enjeu pédagogique majeur.
----------------------------------------------------------------------
Introduction:
Battlefield tourniquet use can be lifesaving, but most reports are from hospitals with knowledge gaps remaining at the forward surgical team (FST). The quality of tourniquet applications in forward settings remain unknown. The purpose of this case series is to describe observations of tourniquet use at an FST in order to improve clinical performance.
Methods:
War casualties with tourniquet use presenting to an FST in Afghanistan in 2011 were observed. We identified appliers by training, device effectiveness, injury pattern, and clinical opportunities for improvement. Feedback was given to treating medics.
Results:
Tourniquet applications (79) were performed by special operations combat medics (47, 59%), flight medics (17, 22%), combat medics (12, 15%), and general surgeons (3, 4%). Most tourniquets were Combat Application Tourniquets (71/79, 90%). With tourniquets in place upon arrival at the FST, most limbs (83%, 54/65) had palpable distal pulses present; 17% were pulseless (11/65). Of all tourniquets, the use was venous in 83% and arterial in 17%. In total, there were 14 arterial injuries, but only 5 had effective arterial tourniquets applied.
Discussion:
Tourniquets are liberally applied to extremity injuries on the battlefield. 17% were arterial and 83% were venous tourniquets. When ongoing bleeding or distal pulses were appreciated, medics tightened tourniquets under surgeon supervision until distal pulses stopped. Medics were generally surprised at how tight a tourniquet must be to stop arterial flow–convert a venous tourniquet into an arterial tourniquet. Implications for sustainment training should be considered with regard to this life-saving skill.
| Tags : tourniquet, garrot, hémorragie
13/01/2015
Attentats: Importance du garrot
The Initial Response to the Boston Marathon Bombing. Lessons Learned to Prepare for the Next Disaster
Gates JD et AL. Ann Surg. 2014 Dec;260(6):960-6
-----------------------------------------------------------------------------------
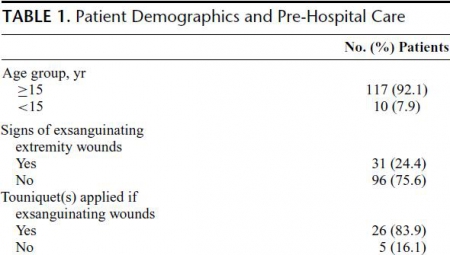
Le concept du garrot tactique est familier aux équipes militaires. L'expérience rapportée montre que ce concept doit également le devenir dans le monde de la médecine préhospitalière. 26 soit près de 10% blessés pris en charge ont fait l'objet d'une pose de garrot. Ainsi en cas d'attentat la pose précoce d'un garrot en cas d'hémorragie des membres est elle une mesure fondamentale de mise en condition de survie.
-----------------------------------------------------------------------------------
OBJECTIVE:
We discuss the strengths of the medical response to the Boston Marathon bombings that led to the excellent outcomes. Potential shortcomings were recognized, and lessons learned will provide a foundation for further improvements applicable to all institutions.
BACKGROUND:
Multiple casualty incidents from natural or man-made incidents remain a constant global threat. Adequate preparation and the appropriate alignment of resources with immediate needs remain the key to optimal outcomes.
METHODS:
A collaborative effort among Boston's trauma centers (2 level I adult, 3 combined level I adult/pediatric, 1 freestanding level I pediatric) examined the details and outcomes of the initial response. Each center entered its respective data into a central database (REDCap), and the data were analyzed to determine various prehospital and early in-hospital clinical and logistical parameters that collectively define the citywide medical response to the terrorist attack.
RESULTS:
A total of 281 people were injured, and 127 patients received care at the participating trauma centers on that day. There were 3 (1%) immediate fatalities at the scene and no in-hospital mortality. A majority of the patients admitted (66.6%) suffered lower extremity soft tissue and bony injuries, and 31 had evidence for exsanguinating hemorrhage, with field tourniquets in place in 26 patients. Of the 75 patients admitted, 54 underwent urgent surgical intervention and 12 (22%) underwent amputation of a lower extremity.
CONCLUSIONS:
Adequate preparation, rapid logistical response, short transport times, immediate access to operating rooms, methodical multidisciplinary care delivery, and good fortune contributed to excellent outcomes.
| Tags : tourniquet, garrot, hémorragie
07/12/2014
Tourniquet: Que disent les utilisateurs ?
Le garrot en dotation dans l'armée française est le Special Operation Tactical Tourniquet (SOFT-T) , concurrent du Combat Application Tourniquet (CAT). Il existe de nombreux travaux qui cherchent à comparer entre eux les divers produits proposés par l'industrie. Tel garrot semble plus efficace sur des modèles expériemetaux, un autre voit sa barre de torsion se briser, un autre est plus fragile que son concurrent lorsque les conditions de stockage ne sont pas optimales.

Une autre démarche consiste à demander à ceux qui les ont employé en conditions réelles. Une idée est donnée par le tableau qui suit et qui est tiré d'un questionnaire de suivi de mise en oeuvre des équipements du TCCC. Le modèle actuellement en dotation apparaît parfaitement adapté.
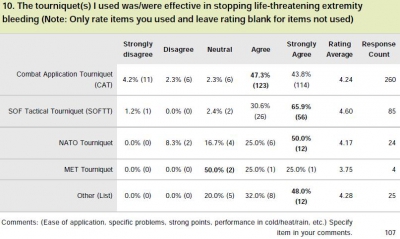
Clic sur l'image pour accéder au suivi des équipemens du TCCC
| Tags : tourniquet
Tourniquet: La largeur compte
Tourniquets and Occlusion: The Pressure of Design
Wall PL et AL. Military Medicine, 178, 5:578, 2013
-------------------------------------------------------------------
Cet article est intéressant car il met en évidence que d'autres garrots que les tourniquets du type du CAT sont efficaces en matière d'occlusion notamment ceux basés sur l'emploi de bandes compressives comme le SWAT-T et d'autre part que le niveau de pression d'occlusion observé avec un tourniquet classique peut être associé à un resaignment si l'on observe un relâchement musculaire
-------------------------------------------------------------------
Nerve injuries result from tourniquet pressure. The objective was to determine arterial occlusion and completion pressures with the 3.8-cm-wide windlass Combat Application Tourniquet (CAT) and the 10.4-cm-wide Stretch, Wrap, and Tuck Tourniquet (SWAT-T). Methods: Sixteen volunteers self-applied and had tourniquets applied to their thighs and arms (CAT and SWAT-T, random order, then blood pressure cuffs). Results: Occlusion (Doppler signal elimination) pressures were higher than predicted ( p < 0.0001), highest with the CAT ( p < 0.0001), and often lower than completion pressures (completion median, range: CAT 360, 147–745 mm Hg; SWAT-T 290, 136–449 mm Hg; cuff 184, 108–281 mm Hg). Three CAT thigh and 9 CAT arm completion pressures were >500 mm Hg. Pressure decreases and occlusion losses occurred over 1 minute (pressure decrease: CAT 44 ± 33 mm Hg; SWAT-T 6 ± 8 mm Hg; cuff 14 ± 19 mm Hg; p < 0.0001; loss/initially occluded: CAT 17 of 61, SWAT-T 5 of 61, cuff 40 of 64, p < 0.01). CAT pressures before turn did not have a clear relationship with turns to occlusion. Conclusions: Limb circumference/ tourniquet width occlusion pressure predictions are not good substitutes for measurements. The wider SWAT-T has lower occlusion and completion pressures than the CAT. Decreases in muscle tension lead to decreases in tourniquet pressure, especially with the nonelastic CAT, which can lead to occlusion loss
| Tags : tourniquet
01/11/2014
Garrot: A partir de quand est on fiable ?
Single versus Double Routing of the Band in the Combat Application Tourniquet.
J Spec Oper Med. 2013 Spring;13(1):34-41.
Le sauvetage au combat met en avant l'importance d'arrêter toute hémorragie le plus tôt possible. Le garrot tient là une place essentielle. Mais à partir de quand l'apprentissage de cette technique peut il être considéré comme optimal. Une réponse est apporté par ce travail: La maîtrise de ce geste semble être obtenue à partir de 30 poses.
Background: Common first aid tourniquets, like the Combat Application Tourniquet (CAT) of a windlass and band design, can have the band routed through the buckle in three different ways, and recent evidence indicates users may be confused with complex doctrine.
Objective: The purpose of the present study is to measure the differential performance of the three possible routings in order to better understand good tourniquet practice.
Methods: A training manikin was used by two investigators to measure tourniquet effectiveness, time to stop bleeding, and blood loss.
Results: The effectiveness rate was 99.6% (239/240) overall. Results were similar for both single-slit routings (inside vs. outside, p > 0.05). Effectiveness rates (yes-no results for hemorrhage control expressed as a proportion of iterations) were not statistically different between single and double routing. However, the time to stop bleeding and blood loss were statistically different (p < 0.05).
Conclusions: CAT band routing, through the buckle either singly or doubly, affects two key performance criteria: time to stop bleeding and volume of blood lost. Single routing proved to be faster, thereby saving more blood. Learning curves required to optimize user performance varied over 30-fold depending on which variable was selected (e.g., effectiveness vs. blood loss).
| Tags : tourniquet
31/10/2014
Garrot: Pas de jeu avant de serrer
No slackers in tourniquet use to stop bleeding
Polston RW et Al. J Spec Oper Med. 2013 Summer;13(2):12-9.
La performance d'un garrot tient pour beaucoup à la manière dont il va être posé. Le garrot en dotation comporte un dispositif de serrage de type tourniquet. L'efficacité de ce dispositif est en grande partie liée à l'absence de jeu au niveau de la sangle du garrot avant le serrage. Il est fondamental de positionner le garrot à la racine du membre, de le mettre en tension manuellement en tirant sur la sangle de façon à effectuer un premier serrage du garrot et ensuite de renforcer ce serrage par la barre du tourniquet. On rappelle qu'en principe l'efficacité est obtenue à partir de 3 tours. (la fiche technique). Le travail présenté ci après est éloquent sur l'intérêt de prohiber tout jeu avec de tourner la barre de torsion.
----------------------------------------------------------------------------------
Background: Tourniquets on casualties in war have been loose in 4%?9% of uses, and such slack risks death from uncontrolled bleeding. A tourniquet evidence gap persists if there is a mechanical slack?performance association.
Objective: The purpose of the present study was to determine the results of tourniquet use with slack in the strap versus no slack before windlass turning, in order to develop best practices. Methods: The authors used a tourniquet manikin 254 times to measure tourniquet effectiveness, windlass turns, time to stop bleeding, and blood volume lost at 5 degrees of strap slack (0mm, 25mm, 50mm, 100mm, and 200mm maximum).
Results: When comparing no slack (0mm) to slack (any positive amount), there were increases with slack in windlass turns (p < .0001, 3-fold), time to stop bleeding (p < .0001, 2-fold), and blood volume lost (p < .0001, 2-fold). When comparing no slack to 200mm slack, the median results showed an increase in slack for windlass turns (p < .0001), time to stop bleeding (p < .0001), and blood volume lost (p < .0001).
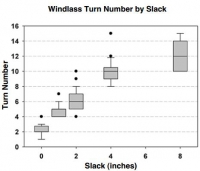
Conclusions: Any slack presence in the strap impaired tourniquet performance. More slack had worse results. Trainers can now instruct tourniquet users with concrete guidance.
| Tags : garrot, tourniquet
Garrot: Comment positionner la boucle ?
Emergency tourniquet effectiveness in four positions on the proximal thigh.
Kragh JF et Al. J Spec Oper Med. 2014 Spring;14(1):26-9.
La procédure du sauvetage au combat précise que le garrot doit être posé à la racine du membre. Elle ne précise cependant pas comment le dispositif de serrage doit être placé: en avant sur le côté en arrière du membre. Ce travail tente de répondre à cette question.
----------------------------------------------------------------------------------
Objective: The purpose of the present study is to determine the performance of tourniquet use by the placement of the tourniquet's windlass on the extremity in four positions: medial, lateral, anterior, and posterior? to inform tourniquet instructors and develop best tourniquet practices.
Methods: A HapMed™ Leg Tourniquet Trainer was used as a manikin to test the effectiveness of an emergency tourniquet, the Special Operations Forces Tactical Tourniquet. Two users made 10 tests, each in four positions.
Results: Effectiveness rates of tourniquet use were 100% in all four positions. The two tourniquet users were both right-hand dominant and used their right hand to turn the windlass. One user turned the windlass clockwise, and the other turned it counterclockwise. The association between time to stop bleeding and tourniquet position was statistically significant but associations between time to stop bleeding and the user, user-by-position, and windlass turn number were not statistically significant. The association between tourniquet position and pressure under the tourniquet was statistically significant, and the association between user and pressure under thetourniquet was statistically significant, but the user-by-position and windlass turn number were not statistically significant. The associations betweentourniquet position and blood loss volume, user and blood loss volume, and user-by-position and blood loss volume were statistically significant. Conclusions: The present study found that tourniquet effectiveness rates were uniformly 100% irrespective of whether the windlass position was medial, lateral, anterior, or posterior. These excellent clinical and statistical results indicate that users may continue to place the tourniquets as they prefer upon the proximal thigh
| Tags : tourniquet, garrot
28/01/2014
The tourniquet manual
Clic sur l'image pour accéder au document
| Tags : tourniquet
06/09/2013
Tourniquet abdominal: Compression axillaire ?

| Tags : tourniquet, hémorragie, jonctionnel
22/07/2013
Tourniquet: Serrer fort et surtout vérifier l'efficacité
Forward Assessment of 79 Prehospital Battlefield Tourniquets Used in the Current War
King DR et All. J Spec Oper Med. 2012 Winter;12(4):33-8.
Un article important qui doit faire réfléchir à la manière dont l'instruction sur le garrot est conduite aussi bien au niveau du SC1 que du SC 2.
Dans ce document il est expliqué que 79 garrots sont posés sur 65 jambes garrotées de 54 combattants. Seules 17 jambes avaient des lésions artérielles. 14 d'entre elles étaient majueres mais seules 4 avait un garrot sérré correctement c'est à dire avec abolition du pouls distal. mais qu'aucune lésion artérielle n'a été prise en charge sans garrot sur la même période. Un rappel simple est fait sen outre sur l'importance de la largeur du garrot.
________________________________________________
Introduction: Battlefield tourniquet use can be lifesaving, but most reports are from hospitals with knowledge gaps remaining at the forward surgical team (FST). The quality of tourniquet applications in forward settings remain unknown. The purpose of this case series is to describe observations oftourniquet use at an FST in order to improve clinical performance.
Methods: War casualties with tourniquet use presenting to an FST in Afghanistan in 2011 were observed. We identified appliers by training, device effectiveness, injury pattern, and clinical opportunities for improvement. Feedback was given to treating medics. Results: Tourniquet applications (79) were performed by special operations combat medics (47, 59%), flight medics (17, 22%), combat medics (12, 15%), and general surgeons (3, 4%). Most tourniquets were Combat Application Tourniquets (71/79, 90%). With tourniquets in place upon arrival at the FST, most limbs (83%, 54/65) had palpable distal pulses present; 17% were pulseless (11/65). Of all tourniquets, the use was venous in 83% and arterial in 17%. In total, there were 14 arterial injuries, but only 5 had effective arterial tourniquetsapplied.
Discussion: Tourniquets are liberally applied to extremity injuries on the battlefield. 17% were arterial and 83% were venous tourniquets. When ongoing bleeding or distal pulses were appreciated, medics tightened tourniquets under surgeon supervision until distal pulses stopped. Medics were generally surprised at how tight a tourniquet must be to stop arterial flow ? convert a venous tourniquet into an arterial tourniquet. Implications for sustainment training should be considered with regard to this life-saving skill.
________________________________________________
1. Les garrots doivent être serrés de manière conforme; arrêt du saignement et dès que possible contrôle de l'absence de pouls.
2. Les garrots doivent être surveillés tout au long de la chaine de prise en charge
3. La fiche mémento sur le concept de garrot tactique est à lire et relire
| Tags : tourniquet, garrot
05/07/2013
Garrot: Une nouvelle ère ?
New Tourniquet Device Concepts for Battlefield Hemorrhage Control
Kragh JF et all.US Army Med Dep J. 2011 Apr-Jun:38-48.
Ground:
Given the recent success of emergency tourniquets, limb exsanguination is no longer the most common cause of preventable death on the battlefield; hemorrhage amenable to truncal tourniquets now is. The purpose of the present study is to discuss the gaps today in battlefield hemorrhage control and candidate solutions in order to stimulate the advancement of prehospital combat casualty care.
Methods:
A literature review, a market survey of candidate devices, a request for devices, and an analysis of the current situation regarding battlefield hemorrhage control were performed.
Results:
Hemorrhage control for wounds in the junction between the trunk and the limbs and neck is a care gap in the current war, and, of these, the pelvic (including buttock and groin proximal to the inguinal ligament) area is the most common. Historical and recent reports give background information indicating that truncal tourniquets are plausible devices for controlling junctional hemorrhage on the battlefield. A request for candidate devices yielded few prototypes, only one of which was approved by the US Food and Drug Administration.
Conclusions:
In order to solve the now most common cause of preventable death on the battlefield, junctional hemorrhage from the pelvic area, the planned approach is a systematic review of research, device and model development, and the fielding of a good device with appropriate training and doctrine.
| Tags : jonctionnel, tourniquet
03/06/2013
Garrots: Sur soi mais pas n'importe comment !
Efficacy of tourniquets exposed to the afghanistan combat environment stored in individual first aid kits versus on the exterior of plate carriers
Weppner J et all. Mil Med. 2013 Mar;178(3):334-7
Between February and May 2010, 1st Battalion, 6th Marines reported a 10% (10/92) breakage rate for tourniquets. One theory suggested was that tourniquets were weakened by exposure to the Afghan environment. Our study was designed to compare three groups of Afghanistan-exposed tourniquets to unexposed tourniquets. The three experimental arms were: (1) Afghan-exposed tourniquets worn on the plate carrier, (2) Afghan-exposed tourniquets carried in the Individual First Aid Kit (IFAK) and wrapped in manufacturer plastic wrapping, and (3) Afghan-exposed tourniquets carried in the IFAK with the manufacturer plastic wrapping removed. The outcome measures of this study were efficacy, breakage, and number of turns required to successfully stop the distal pulse. Tourniquets worn on the plate carrier had an efficacy of 57%, which was significantly lower than the control efficacy rate of 95.2%. When compared to the control arm, there were no significant differences in efficacy between the tourniquets stored in the IFAK with or without manufacturing packaging. No control tourniquets or tourniquets stored in IFAKs broke; however, 46 (12%) of the plate carrier-exposed tourniquets did break. No statistically significant differences were found between the four groups with regard to the median number of turns required to stop the distal pulse.
| Tags : tourniquet
02/06/2013
Hémorragies jonctionnelles: Comprimer le pelvis
UK Combat-Related Pelvic Junctional Vascular Injuries 2008-2011: Implications for Future Intervention.
Walker NM et All. - Bone Joint Journal (2013) vol. 95-B no. SUPP 8 13
---------------------------------------------------------------------------------------
L'arrêt d'une hémorragie jonctionnelle est un enjeu majeur. Plusieurs dispositifs ont été récemment proposés. Il semble que la grande majorité des lésions observées se situent au dessus du ligament inguinal rendant ainsi l'efficacité de dispositif comme le CRoC limité. Le tourniquet abdominal ou le sam junctionnal tourniquet paraissent ainsi au moins théoriquement un meilleur choix si toutefois ils permettent une compression suffisante.
---------------------------------------------------------------------------------------
In a recent publication, 4.6% of 6450 Coalition deaths over ten years were reported to be due to junctional bleeding. The authors suggested that some of these deaths could have been avoided with a junctional hemorrhage control device.
Prospectively collected data on all injuries sustained in Afghanistan by UK military personnel over a 2 year period were reviewed. All fatalities with significant pelvic injuries were identified and analysed, and the cause of death established.
Significant upper thigh, groin or pelvic injuries were recorded in 124 casualties, of which 92 died. Pelvic injury was the cause of death in 42; only 1 casualty was identified where death was at least in part due to a vascular injury below the inguinal ligament, not controlled by a tourniquet, representing <1% of all deaths. Twenty one deaths were due to vascular injury between the aortic bifurcation and the inguinal ligament, of which 4 survived to a medical facility.
Some potentially survivable deaths due to exsanguination may be amenable to more proximal vascular control. We cannot substantiate previous conclusions that this can be achieved through use of a groin junctional tourniquet. There may be a role for more proximal vascular control of pelvic bleeding.
| Tags : tourniquet, hémorragie, jonctionnel