29/10/2013
Intubation en préhospitalier : intérêt des nouvelles techniques
IOT difficile et les nouveaux outils en situation d’urgence ( où en est-on ? )
Les procédures validées
Combes X et All. Urgences - 2013
Points essentiels
■ L’intubation en séquence rapide est la technique de sédation validée pour faciliter l’intubation en situation d’urgence.
■ La préoxygénation peut être réalisée par VNI chez le patient coopérant.
■ Les lames de laryngoscopes en plastique ne doivent pas être utilisées.
■ L’utilisation du mandrin long béquillé est parfaitement validée en situation d’urgence en cas d’intubation difficile sans difficulté de ventilation associées.
■ Le masque laryngé d’intubation Fastrach® est le dispositif de ventilation le plus utile en situation d’urgence.
■ Les vidéolaryngoscopes ne sont pas encore validées pour la prise en charge de l’intubation difficile en situation d’urgence.
■ Les dispositifs de cricothyroïdotomiee basée sur la technique de Seldinger sont à privilégier en situation d’urgence
| Tags : airway, intubation
26/10/2013
Mal des montagnes: Actualisation
| Tags : montagne
L'intraosseuse: Pas adaptée au dammage control resuscitation?
What is the evidence of utility for intraosseous blood transfusion in damage-control resuscitation ?
Harris M et all. J Trauma Acute Care Surg. 2013 Nov;75(5):904-6
« The scientific and clinical evidence for the use of IO access is voluminous, as evidenced by the Scientific Bibliography provided by VidaCare,6 one of the large manufacturers of IO devices, and available in any routine literature search. However direct scientific and/or clinical data to support the use of IO access for the purpose of blood transfusion in adult humans are very limited to anecdotal reports.
the absence of good evidence supporting the use of IO access for the very critical function of blood transfusion in DCR places existing recommendations for its use in question. This lack of evidence is compounded by the clinical experience of the lead author. Multiple attempts to use IO access for blood transfusion, both in the civilian adult emergency setting and in combat casualty care, have repeatedly been unsuccessful »
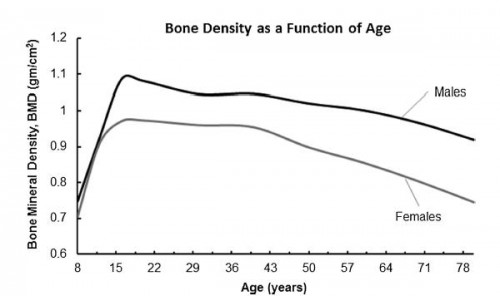
1. La densité osseuse dépend de l'âge
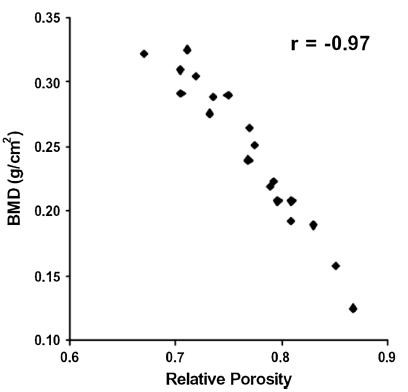
2. La porosité osseuse dépend de la densité osseuse
 77
77
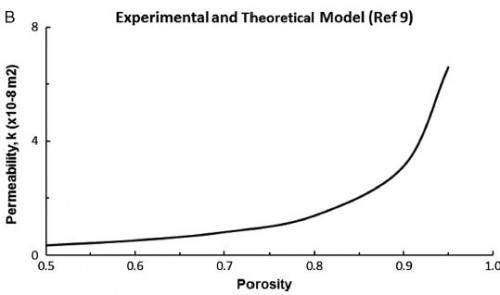
3. La perméabilité osseuse dépend de la porosité
« The bone mineral density increases with age up to a peak density occurring in the early 20s. The soldier population is aged right at the peak of bone density for all races and sex.
the viscosity of pRBCs used in DCR is estimated to be greater than 10 cP.12 Since pRBCs are 10+ times more viscous than crystalloid solutions, it will require at least 10+ times the pressure to obtain the same flow rate as crystalloid in IO infusion.
Based on the Darcy’s Law, the only parameter a medical practitioner has to adjust to increase flow rate in an IO system in DCR is pressure. Increases in pressure not only strain the connections in the infusion system itself but also increase shearing forces in the fluid. Shearing forces may cause hemolysis of the transfused blood, loss of oxygen carrying capacity, and consequent development of rhabdomyolysis
we postulate that maximum flow rates attainable for transfusion of blood products used in DCR via the IO route are simply inadequate for successful resuscitation »
| Tags : intraosseux
20/10/2013
Traumatologie de la main: Anatomie
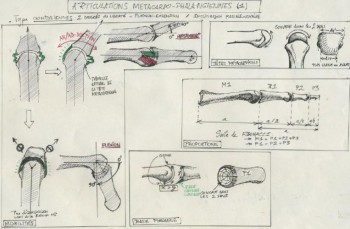
(clic sur l'image pour accéder au document expliquant les bases anatomiques de l'examen d'une main)
18/10/2013
Simulation: Et le modèle animal ?
Use of Animals by NATO Countries in Military Medical Training Exercises: An International Survey
Gala SG et all. Military Medicine, 177, 8:907, 2012
La formation de nos personnels au sauvetage au combat fait appel de multiples ressources pédagogiques. Le recours à des mannequins plus ou moins sophistiqués est de plus en plus courant. Le modèle animal est toujours d'actualité bien que de plus en plus décrié et encadré. Cet article fait le point sur le recours à un tel modèle par les armées de l'OTAN.
| Tags : pédagogie
15/10/2013
Dehors et dedans, ce n'est pas la même chose
Primary blast lung injury prevalence and fatal injuries from explosions: Insights from postmortem computed tomographic analysis of 121 improvised explosive device fatalities
SIngleton JAG et all. J Trauma Acute Care Surg. 2013;75: S269-S274.
BACKGROUND:
Primary blast lung injury (PBLI) is an acknowledged cause of death in explosive blast casualties. In contrast to vehicle occupants following an in-vehicle explosion, the injury profile, including PBLI incidence, for mounted personnel following an external explosion has yet to be as well defined.
METHODS:
This retrospective study identified 146 cases of UK military personnel killed by improvised explosive devices (IEDs) between November 2007 and July 2010. With the permission of Her Majesty's Coroners, relevant postmortem computed tomography imaging was analyzed. PBLI was diagnosed by postmortem computed tomography. Injury, demographic, and relevant incident data were collected via the UK Joint Theatre Trauma Registry.
RESULTS:
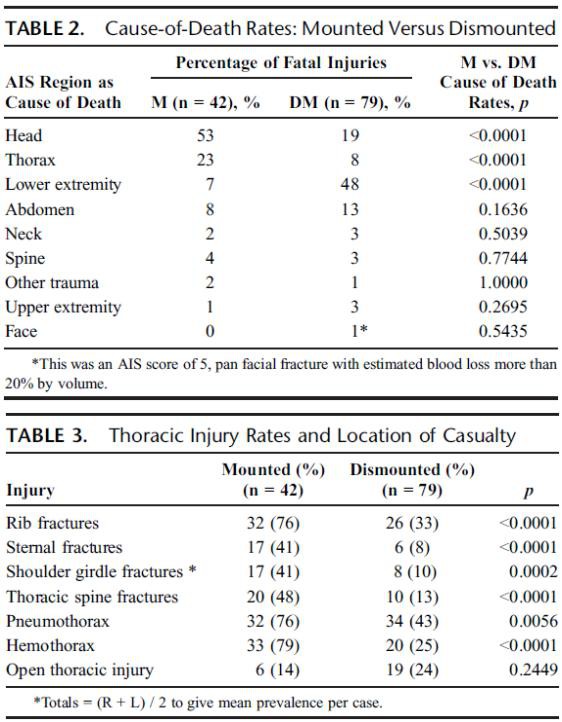
Autopsy results were not available for 1 of 146 cases. Of the remaining 145 IED fatalities, 24 had catastrophic injuries (disruptions), making further study impossible, leaving 121 cases; 79 were dismounted (DM), and 42 were mounted (M). PBLI was noted in 58 cases, 33 (79%) of 42 M fatalities and 25 (32%) of 79 DM fatalities (p < 0.0001). Rates of associated thoracic trauma were also significantly greater in the M group (p < 0.006 for all). Fatal head (53% vs. 23%) and thoracic trauma (23% vs. 8%) were both more common in the M group, while fatal lower extremity trauma (7% vs. 48%) was more commonly seen in DM casualties (p < 0.0001 for all).
CONCLUSION:
Following IED strikes, mounted fatalities are primarily caused by head and chest injuries. Lower extremity trauma is the leading cause of death in dismounted fatalities. Mounted fatalities have a high incidence of PBLI, suggesting significant exposure to primary blast. This has not been reported previously. Further work is required to determine the incidence and clinical significance of this severe lung injury in explosive blast survivors. In addition, specific characteristics of the vehicles should be considered.
| Tags : blast, balistique
09/10/2013
Aide cognitive: Pour gérer une situation de crise
Gérer une situation de crise ne s'improvise pas (CRM: Crisis ressources management). Ceci nécessite la mise en oeuvre de ressources complexes parfaitement décrite dans la figure qui suit et qui doit être bien comprise pour la mise en oeuvre d'un poste de secours.
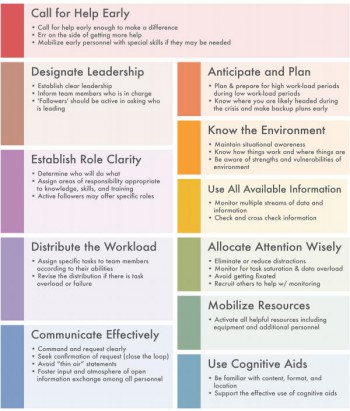
L'université de Stanford fait la promotion de l'emploi de telles aides accessibles sur ce lien. De telles aides sont également proposées par la SFAR. On peut estimer que la fiche RSA peut être assimilé à une aide cognitive pre et post management CRM.
02/10/2013
Mental health following traumatic physical injury: An integrative literature review
Mental health following traumatic physical injury: An integrative literature review
Wiseman T et All. Injury, Int. J. Care Injured 44 (2013) 1383–1390
A B S T R A C T
Aim: To investigate the state of knowledge on the relationship between physical trauma and mental health in patients admitted to hospital with traumatic physical injury.
Background: Adults who sustain traumatic physical injury can experience a range of mental health problems related to the injury and subsequent changes in physical health and function. However earlyscreening and identification of mental health problems after traumatic physical injury is inconsistent and not routine during the hospital admission process for the physically injured patient.
Methods:
Integrative review methods were used. Data were sourced for the period 1995–2010 fromEMBASE, CINAHL, MEDLINE and PsycINFO and hand searching of key references. Abstracts were screened by 3 researchers against inclusion/exclusion criteria. Forty-one papers met the inclusion criteria. Data were retrieved, appraised for quality, analysed, and synthesised into 5 main categories.
Results: Forty-one primary research papers on the relationship between mental health and traumatic physical injury were reviewed. Studies showed that post-traumatic stress disorder, depression and anxiety were frequent sequelae associated with traumatic physical injury. However, these conditions were poorly identified and treated in the acute hospital phase despite their effect on physical health.
Conclusion: There is limited understanding of the experience of traumatic physical injury, particularly in relation to mental health. Greater translation of research findings to practice is needed in order to promote routine screening, early identification and referral to treatment for mental health problems in this patient group.
| Tags : psychiatrie, ptsd
01/10/2013
Infection in conflict wound
Infection in conflict wound
Eardley WGP et All. Phil. Trans. R. Soc. B (2011) 366, 204–218
Although mechanisms of modern military wounding may be distinct from those of ancient conflicts, the infectious sequelae of ballistic trauma and the evolving microbial flora of war wounds remain a considerable burden on both the injured combatant and their deployed medical systems. Battlefieldsurgeons of ancient times favoured suppuration in war wounding and as such Galenic encouragement of pus formation would hinder progress in wound care for centuries. Napoleonic surgeonseventually abandoned this mantra, embracing radical surgical intervention, primarily by amputation, to prevent infection. Later, microscopy enabled identification of microorganisms and characterization of wound flora. Concurrent advances in sanitation and evacuation enabled improved outcomes and establishment of modern military medical systems. Advances in medical doctrine and technology afford those injured in current conflicts with increasing survivability through rapid evacuation, sophisticated resuscitation and timely surgical intervention. Infectious complications in those that do survive, however, are a major concern. Addressing antibiotic use, nosocomial transmission and infectious sequelae are a current clinical management and research priority and will remain so in an era characterized by a massive burden of combat extremity injury. This paper provides a review of infection in combat wounding from a historical setting through to the modern evidence base.
| Tags : infection