
Background
Patients and methods
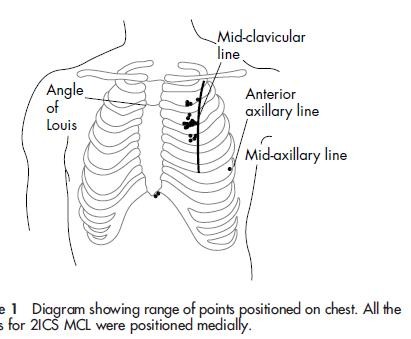
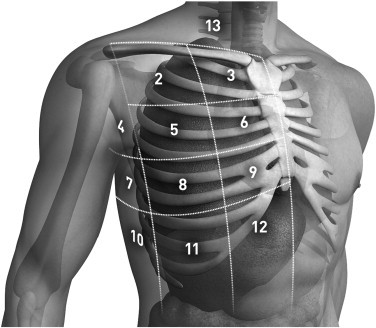
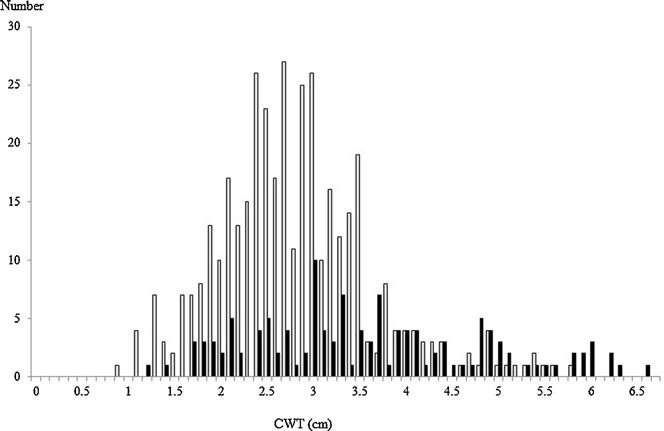
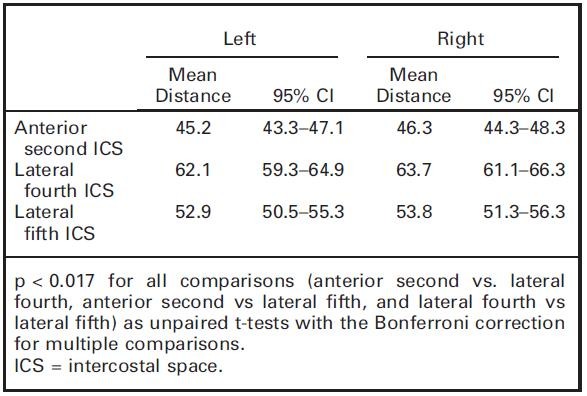
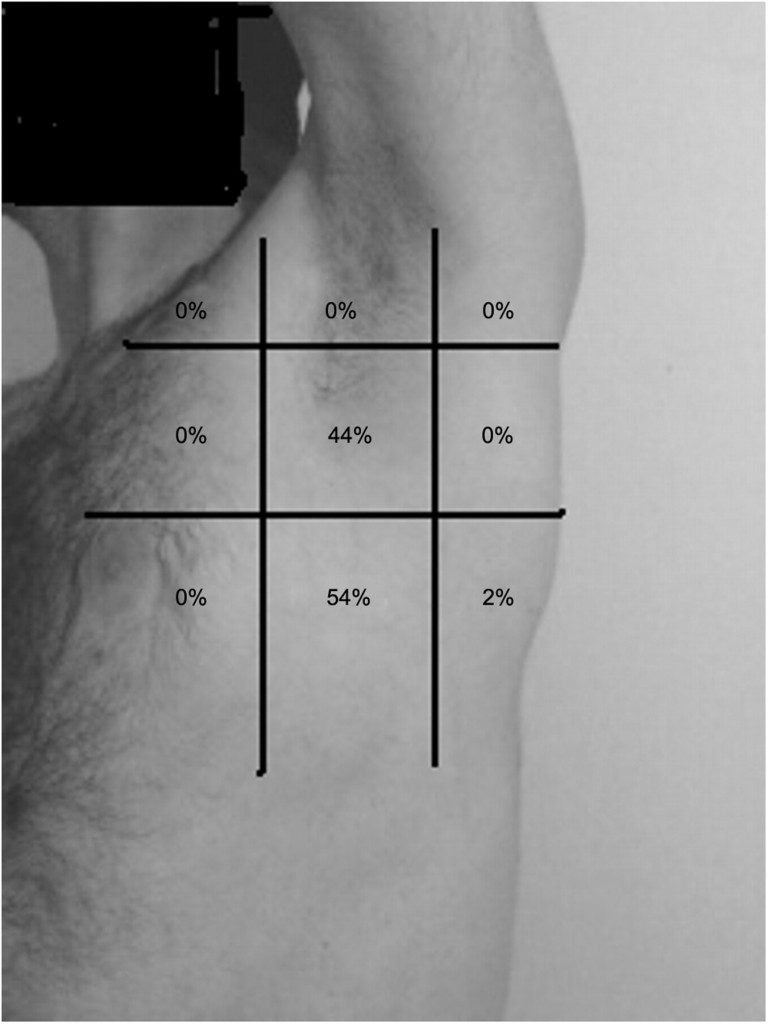
We performed a retrospective review of chest computed tomography of 256 adult Japanese trauma patients who were admitted to the level 1 trauma centre of Tokai University Hospital in Kanagawa, Japan between January and July 2008. In 256 patients, the CWT at 512 sites (left and right sides) was measured by chest computed tomography at the second intercostal space in the middle clavicular line. The frequency of measurement sites <5.0 cm was calculated simultaneously.
The samples were divided according to gender, side (left and right), abbreviated injury scale (<3, ≧3), arm position during examination (up/down), and the existence or non-existence of associated injuries (pneumothorax, subcutaneous emphysema, and fracture of the sternum and ribs); the CWT of each group was compared.
Results
The mean CWT measured in 192 males and 64 females was 3.06 ± 1.02 cm. The CWT values at 483 sites (94.3%) were less than 5.0 cm. The CWT of females was significantly greater than that of males (3.66 cm vs. 2.85 cm, p < 0.0001), and patients with subcutaneous emphysema had greater CWTs than those without it (4.16 cm vs. 3.01 cm, p < 0.0001).
Conclusion
The mean CWT at the second intercostal space in the middle clavicular line was 3.06 cm. It is likely that over 94% of Japanese trauma patients could be treated with a 5.0-cm catheter.