16/07/2013
Management of bleeding and coagulopathy following major trauma: an updated European guideline
| Tags : hémorragie, traumatologie
29/06/2013
Coagulopathie du trauma: Que faire ?
Case Scenario: Management of Trauma-induced Coagulopathy in a Severe Blunt Trauma Patient
David JS et All. Anesthesiology 2013; 119:191–200
Un point très clair du problème
| Tags : coagulopathie
02/12/2012
Hémostase et transfusion par A. Godier IAR IDF

CLIC sur le logo pour accéder au cours
| Tags : hémorragie
Choc hémorragique par D. Journois IAR IDF
CLIC sur le logo pour visualiser le cours
| Tags : choc, hémorragie, remplissage
01/12/2012
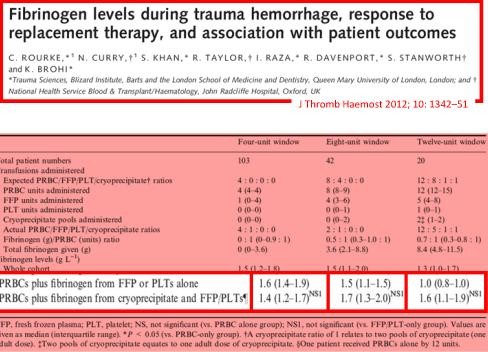
Apport du fibrinogène: A la folie ou pas du tout ??
Une econférence qui fait parfaitement le point sur l'intérêt et les questions en suspens concernant l'intérêt du fibrinogène dans la réanimation hémostatique du traumasié qui saigne.
En condition de combat avant l'arivée en structure hopsitalière de campagne, l'apport de fibrinogène peut être réalisé par l'apport de plasma lyophylisé (PLYO) produit par le SSA (obtenu en moins de 6 min après reconstitution à température ambiante par adjonction d'eau PPI, chaque unité contient au moins 0,5g de fibrinogène). C'est une des composantes de la transfusion de plasma thérapeutique. qui doit désormais être envisagé au niveau du role 1 (poste de secours ou vecteur d'évacuation tactique).
Le recours au fibrinogène (Clottafact), qui apparaît être d'un intérêt majeur compte tenu d'un apport insuffisant par la transfusion de plasma. (Abstract Rourke et all.)
Il ne peut (pour des raisons de logistique de production et de disponibilté) être apporté qu'à partir de la prise en charge hospitalière.
Pour approfondir avec en perspective le blessé de guerre hémorragique:
(1) Un revue générale sur la coagulopathie de l'hémorragie massive: "Hemodilution caused by trauma and major surgery induces complex hemostatic changes involving procoagulant factors as well as anticoagulant, fibrinolytic, and antifibrinolytic factors. The endothelial responses to shear stress, active proteases, and various inflammatory cells and cytokines add further complexity to the pathophysiology of massive hemodilution. In addition to the conventional transfusion products, which are often difficult to administer in a timely manner, purified factor concentrates of plasma origin and from recombinant synthesis are highly concentrated (i.e., small volume) for a rapid restoration of targeted factor(s). The use of point-of-care testing is desirable to optimize the dose and timing of such intervention. Additional clinical trials of different factor concentrate therapies are required to validate their efficacy and safety in patients after trauma or major surgery.152 Further understanding of the time course of pathophysiological changes in massive hemodilution is necessary to optimally balance hemostatic and anticoagulant therapies."
(2) Un focus sur le blessé de guerre: "In patients with combatrelated trauma requiring massive transfusion, the transfusion of an increased fibrinogen: RBC ratio was independently associated with improved survival to hospital discharge, primarily by decreasing death from hemorrhage. Prospective studies are needed to evaluate the best source of fibrinogen and the optimal empiric ratio of fibrinogen to RBCs in patients requiring massive transfusion."
(3) La stratégie transfusionnelle du blessé de guerre SFAR 2012: " En traumatologie, l’administration de fibrinogène est recommandée : dose initiale de 3 à 4 g suivie d’une administration régulière en cas d’hypofibrinogènémie biologique (<1,5 à 2 g/l) ou de signes thromboelastométriques de déficit fonctionnel en fibrinogène [8]. Une analyse nord-américaine rétrospective de 252 dossiers de BdG ayant nécessité une TM a permis de mettre en évidence qu’un apport faible de fibrinogène (< 0,2 g/CGR) au cours de la transfusion était associé à une majoration significative de la mortalité de ces blessés [39]. Le SSA américain utilise l’apport de cryoprécipités contenant surtout du fibrinogène et d’autres facteurs de coagulation pour compenser ces déficits [37]. Les recommandations du SSA français sont l’administration de fibrinogène de façon répétée afin de maintenir un fibrinogène plasmatique supérieur à 1,5 g/l ou en l’absence de laboratoire (situation des structures chirurgicales « légères »), d’administrer au moins 0,2 g de fibrinogène par CGR transfusé."
| Tags : coagulopathie
23/09/2012
Facteur VIIa: Intérêt pas prouvé !
Use of recombinant factor VIIA for control of combat-related haemorrhage.
Woodruff SI et all. Emerg Med J 2010;27:2 121-124
Ce travail met en exergue que le recours au FVIIa n'a pas d'intérêt prouvé en cas de prise en charge de traumatismes pénétrants. Ceci est d'autant plus vrai qu'il est fait alors qu'une coagulopathie sévère est installée (The utility of recombinant factor VIIa as a last resort in trauma. Mamtani R. et all. World Journal of Emergency Surgery 2012, 7(Suppl 1):S7)
----------------------------------------------
Background
Recombinant activated human coagulation factor VII (rFVIIa), an intravascular strategy to promote clotting, is being used as an adjunct to surgical control of bleeding in combat trauma patients.
Objective
To describe the initial experiences with rFVIIa administered to combat casualties at US Navy-Marine Corps medical treatment facilities in Iraq, and to comparesurvival outcomes of those treated with rFVIIa to controls not receiving rFVIIa.
Methods
Medical encounter data from the US Navy-Marine Corps Combat Trauma Registry were retrospectively reviewed to identify all battle-injured patients documented as having received rFVIIa during the period May 2004 to January 2006 of Operation Iraqi Freedom. Available clinical and injury related data are presented to characterise the patients. To assess effects of rFVIIa on survival outcomes, rFVIIa cases were matched to controls on injury severity and age.
Results
22 battle-injured patients from the Combat Trauma Registry received rFVIIa. Primarily young US Marines, these patients typically had penetrating injuries from improvised explosive devices and gunshot wounds. Injuries were often abdominal. The average dose used was similar to that reported in another study of civilian trauma patients, although dosing varies widely in the existing experimental and anecdotal literature. Over two-thirds (68%) of the rFVIIa patients surviveddan identical outcome seen for a matched control group of 22 patients.
Conclusions
Survival of seriously injured combat casualties was good, although identical to that of a control group. Methodological limitations of this retrospective study preclude making firm conclusions about the effectiveness of rFVIIa. Future controlled studies are needed for safety and efficacy testing of rFVIIa in combat trauma patients.
----------------------------------------------
| Tags : hémorragie, coagulopathie
29/03/2011
Exacyl: OUI mais dans l'heure qui suit le trauma
L'exacyl est recommandé pour la prise en charge du traumatisé. L'étude Crash 2 l'a montré. Un complément d'analyse de cette étude précise cependant qu'il faut l'administer dans l'heure suivant le traumatisme.
---------------------------------------------------------------
The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial
Findings
Interpretation