09/10/2016
Blessés des combats modernes:Spécifiques
A modern combat trauma
INTRODUCTION:
The world remains plagued by wars and terrorist attacks, and improvised explosive devices (IED) are the main weapons of our current enemies, causing almost two-thirds of all combat injuries. We wished to analyse the pattern of blast trauma on the modern battlefield and to compare it with combat gunshot injuries.
MATERIALS AND METHODS:
Analysis of a consecutive series of combat trauma patients presenting to two Bulgarian combat surgical teams in Afghanistan over 11 months. Demographics, injury patterns and Injury Severity Scores (ISS) were compared between blast and gunshot-injured casualties using Fisher's Exact Test.
RESULTS:
The blast victims had significantly higher median ISS (20.54 vs 9.23) and higher proportion of ISS>16 (60% vs 33.92%, p=0.008) than gunshot cases. They also had more frequent involvement of three or more body regions (47.22% vs 3.58%, p<0.0001). A significantly higher frequency of head (27.27% vs 3.57%), facial (20% vs 0%) and extremities injuries (85.45% vs 42.86%) and burns (12.72% vs 0%) was noted among the victims of explosion (p<0.0001). Based on clinical examination and diagnostic imaging, primary blast injury was identified in 24/55 (43.6%), secondary blast injury in 37 blast cases (67.3%), tertiary in 15 (27.3%) and quaternary blast injury (all burns) in seven (12.72%).
CONCLUSIONS:
Our results corroborate the 'multidimensional' injury pattern of blast trauma. The complexity of the blast trauma demands a good knowledge and a special training of the military surgeons and hospital personnel before deployment.
| Tags : blast
17/06/2016
Protection: Hauteur du tronc plutôt que taille
Determining the dimensions of essential medical coverage required by military body armour plates utilising Computed Tomography
Breeze J et Al. http://dx.doi.org/10.1016/j.injury.2016.06.010
Plus que la taille du combattant, c'est la hauteur du thorax qui doit guider le choix des protections ballistiques du tronc
-------------------------------------------
Introduction
Military body armour is designed to prevent the penetration of ballistic projectiles into the most vulnerable structures within the thorax and abdomen. Currently the OSPREY and VIRTUS body armour systems issued to United Kingdom (UK) Armed Forces personnel are provided with a single size front and rear ceramic plate regardless of the individual’s body dimensions. Currently limited information exists to determine whether these plates overprotect some members of the military population, and no method exists to accurately size plates to an individual.
Method
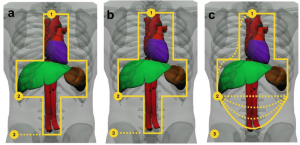
Computed Tomography (CT) scans of 120 male Caucasian UK Armed Forces personnel were analysed to measure the dimensions of internal thoraco-abdominal anatomical structures that had been defined as requiring essential medical coverage. The boundaries of these structures were related to three potential anthropometric landmarks on the skin surface and statistical analysis was undertaken to validate the results.
Results The range of heights of each individual used in this study was comparable to previous anthropometric surveys, confirming that a representative sample had been used. The vertical dimension of essential medical coverage demonstrated good correlation to torso height (suprasternal notch to iliac crest) but not to stature (r2=0.53 versus 0.04). Horizontal coverage did not correlate to either measure of height. Surface landmarks utilised in this study were proven to be reliable surrogate markers for the boundaries of the underlying anatomical structures potentially requiring essential protection by a plate.
Front and rear Osprey shape
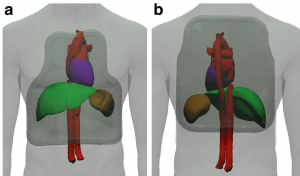
Potential new Shape
Conclusions
Providing a range of plate sizes, particularly multiple heights, should optimise the medical coverage and thus effectiveness of body armour for UK Armed Forces personnel. The results of this work provides evidence that a single width of plate if chosen correctly will provide the essential medical coverage for the entire military population, whilst recognising that it still could overprotect the smallest individuals. With regards to anthropometric measurements; it is recommended, based on this work, that torso height is used instead of stature for sizing body armour. Coverage assessments should now be undertaken for side protection as well as for other non-Caucasian populations and females, with anthropometric surveys utilising the three landmarks recommended in this study.
05/06/2016
40 years of terrorist bombings
40 years of terrorist bombings – A meta-analysis of the casualty and injury profile
Ewards DS et Al. Injury, Int. J. Care Injured 47 (2016) 646–652
Introduction: Terrorists have used the explosive device successfully globally, with their effects extending beyond the resulting injuries. Suicide bombings, in particular, are being increasingly deployed due to the devastating effect of a combination of high lethality and target accuracy. The aim of this study was to identify trends and analyse the demographics and casualty figures of terrorist bombings worldwide.
Methods: Analysis of the Global Terrorism Database (GTD) and a PubMed/Embase literature search (keywords ‘‘terrorist’’, and/or ‘‘suicide’’, and/or ‘‘bombing’’) from 1970 to 2014 was performed.
Results: 58,095 terrorist explosions worldwide were identified in the GTD. 5.08% were suicide bombings. Incidents per year are increasing (P < 0.01). Mean casualty statistics per incidents was 1.14 deaths and 3.45 wounded from non-suicide incidents, and 10.16 and 24.16 from suicide bombings (p < 0.05). The kill:wounded ratio was statistically higher in suicide attacks than non-suicide attacks, 1:1.3 and 1:1.24 respectively (p < 0.05). The Middle East witnessed the most incidents (26.9%), with Europe (13.2%) ranked 4th. The literature search identified 41 publications reporting 167 incidents of which 3.9% detailed building collapse (BC), 60.8% confined space (CS), 23.5% open space (OS) and 11.8% semiconfined space (SC) attacks. 60.4% reported on suicide terrorist attacks. Overall 32 deaths and 180 injuries per incident were seen, however significantly more deaths occurred in explosions associated with a BC. Comparing OS and CS no difference in the deaths per incident was seen, 14.2(SD 17.828) and 15.63 (SD 10.071) respectively. However OS explosions resulted in significantly more injuries, 192.7 (SD 141.147), compared to CS, 79.20 (SD 59.8). Extremity related wounds were the commonest injuries seen (32%).
Discussion/Conclusion: Terrorist bombings continue to be a threat and are increasing particularly in the Middle East. Initial reports, generated immediately at the scene by experienced coordination, on the type of detonation (suicide versus non-suicide), the environment of detonation (confined, open, building collapse) and the number of fatalities, and utilising the Kill:Wounded ratios found in this meta-analysis, can be used to predict the number of casualties and their likely injury profile of survivors to guide the immediate response by the medical services and the workload in the coming days.
20/03/2016
Blessés par balle: Civil et guerre, différent !
17/07/2015
Protection ballistique et exposition céphalique ?
Combat Body Armor and Injuries to the Head, Face, and Neck Region: A Systematic Review
Tong D et Al. Mil Med. 2013 Apr;178(4):421-6
There has been a reported increase in combat-related head, face, and neck (HFN) injuries among service personnel wearing combat body armor (CBA) that have deployed to Iraq and Afghanistan. Modern ceramic plate CBA has decreased the incidence of fatal-penetrating injuries to the torso but offers no protection to the limbs and face which remain exposed to gunshot wounds and fragments from explosive devices. The aim of this review was to systematically summarize the literature reporting on HFN injuries sustained by combat personnel wearing CBA and to highlight recommendations for increased protection to the facial region. Three major contributing factors were identified with this proportional increase in HFN injuries, namely the increased survivability of soldiers because of CBA, fragments injuries from explosive devices, and the lack of protection to the face and limbs. There appears to be no evidence to suggest that by virtue of wearing CBA the likelihood of sustaining an HFN injury increases as such, but a higher incidence of fragment injuries to the HFN region may be due to the more common use of improvised explosive devicess and other explosive devices. Further development of lightweight protection for the face is needed.
28/03/2015
Blast et squelette osseux: Lésions spécifiques ?
Blast Injury and the Human Skeleton: An Important Emerging Aspect of Conflict-Related Trauma.
Dussault C. et Al. J Forensic Sci. 2014 May;59(3):606-12 [Thèse]
--------------------------------------------------------------------
La rupture de la membrane du tympan en cas serait un marqueur peu fiable du blast et de sa gravité (1,2, 3). Il semblerait que certaines lésions osseuses soient assez spécifiques de blast osseux. Ceci a son intérêt en médecine médico-légale quand les circonstances de décès ne sont pas connues.
--------------------------------------------------------------------
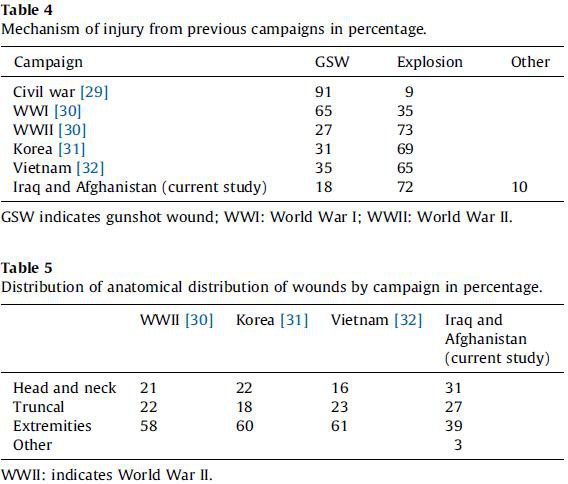
Recent decades have seen an accelerating trend in warfare whereby a growing proportion of conflict-related deaths have been caused by explosions. Analysis of blast injury features little in anthropological literature. We present a review of clinical literature that includes prevalence of injury to anatomical regions and potential indicators of blast injury which can be used by forensic anthropologists. This includes high prevalence of extremity (22.8–91.2%) and facial (19.6–40%) injury in combat contexts, lower limb fractures (19–74.3%) in suicide bombing, traumatic amputation (3–43%) and diffuse fracture patterns in terrorist bombings. Potential indicators of blast trauma include blowout fractures in sinus cavities from blast overpressure, transverse mandibular fractures, and visceral surface rib fractures. Ability to recognize blast trauma and distinguish it in the skeleton is of importance in investigations and judicial proceedings relating to war crimes, terrorism, and human rights violations and likely to become increasingly crucial to forensic anthropology knowledge.
--------------------------------------------------------------------
1. Les factures mandibulaires transverses
[Mandibular fractures in British military personnel secondary to blast trauma sustained in Iraq and Afghanistan. Breeze et al. Br J Oral Maxillofac Surg. 2011 Dec;49(8):607-11]
Elles portent essentiellement sur la symphyse et le corps alors qu'en traumatologie civile il s'agit essentiellement d'atteintes du condyle et de l'angle
2. Les fractures de plancher de type "Blow out"
Le cadre orbitaire reste intact. Le plancher de l'orbite est atteint. Il y a irruption du contenu orbitaire dans le sinus. Le risque est que ces fractures passent inaperçues. Cliniquement elle se traduise par une anomalie de l'occulomotricité.
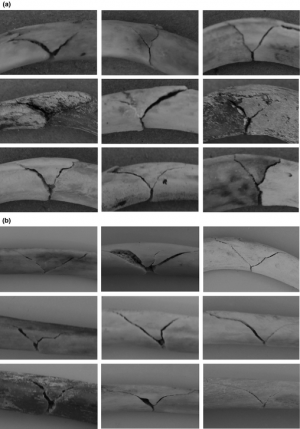
3. Les fractures de cotes en aile de papillon
[Rib Butterfly Fractures as a Possible Indicator of Blast Trauma. Christensen et Al. J Forensic Sci. 2013 Jan;58 Suppl 1:S15-9.]

| Tags : blast
11/01/2015
Histoire de casque de protection
Ballistic helmets – Their design, materials, and performance against traumatic brain injury
Kulkarni SG et Al. Composite Structures 101 (2013) 313–331
Protecting a soldier’s head from injury is critical to function and survivability. Traditionally, combat helmets have been utilized to provide protection against shrapnel and ballistic threats, which have reduced head injuries and fatalities. However, home-made bombs or improvised explosive devices (IEDs) have been increasingly used in theatre of operations since the Iraq and Afghanistan conflicts. Traumatic brain injury (TBI), particularly blast-induced TBI, which is typically not accompanied by external body injuries, is becoming prevalent among injured soldiers. The responses of personal protective equipment, especially combat helmets, to blast events are relatively unknown. There is an urgent need to develop head protection systems with blast protection/mitigation capabilities in addition to ballistic protection.
Modern military operations, ammunitions, and technology driven war tactics require a lightweight headgear that integrates protection mechanisms (against ballistics, blasts, heat, and noise), sensors, night vision devices, and laser range finders into a single system.
The current article provides a comparative study on the design, materials, and ballistic and blast performance of the combat helmets used by the US Army based on a comprehensive and critical review of existing studies. Mechanisms of ballistic energy absorption, effects of helmet curvatures on ballistic performance, and performance measures of helmets are discussed. Properties of current helmet materials (including Kevlar K29, K129 fibers and thermoset resins) and future candidate materials for helmets (such as nano-composites and thermoplastic polymers) are elaborated. Also, available experimental and computational studies on blast-induced TBI are examined, and constitutive models developed for brain tissues are reviewed. Finally, the effectiveness of current combat helmets against TBI is analyzed along with possible avenues for future research.
| Tags : balistique, blast, tbi
12/06/2014
Traumatisé de guerre: Cela évolue
Systematic review of the prevalence and characteristics of battle casualties from NATO coalition forces in Iraq and Afghanistan
Hoencamp R. et All. Injury, Int. J. Care Injured 45 (2014) 1028–1034
23/02/2014
Mousses auxétiques: Encore mieux protégés !
Literature Review: Materials with Negative Poisson's Ratios and Potential Applications to Aerospace and Defence
Liu Q. DSTO Defence Science and Technology Organisation
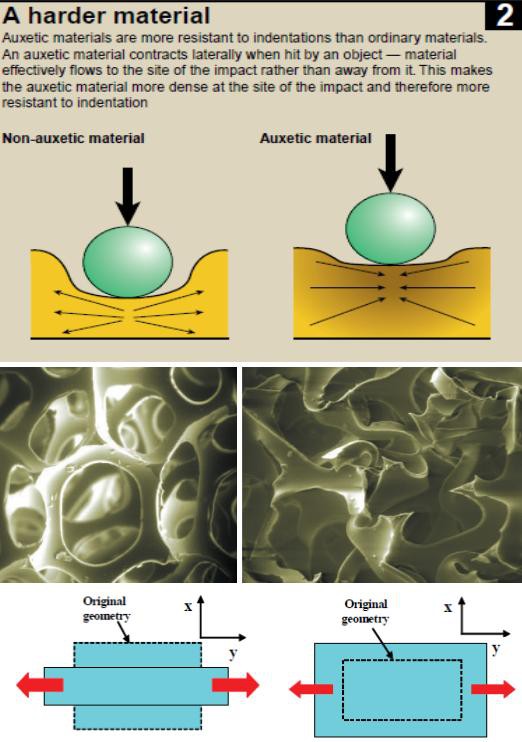
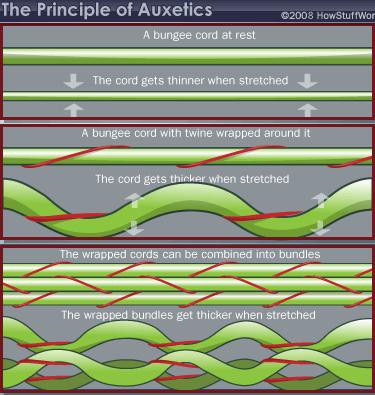
De nombreuse recherches portent sur l'amélioration des effets de protection. Le recours à de nouvelles fibres, le mode de tissage, l'emploi de plaques de céramique permettent actuellement de disposer d' équipements efficaces. Le recours aux nanoparticules est actuellement une voie de recherche, mais ce n'est pas la seule. De nouveaux matériaux ayant la propriété d'augmenter de volume quand ils sont étirés ou soumis à une pression sont utilisables. Ces matériaux sont des mousses dites auxétiques.
03/11/2013
The army hearing program
Heritage of army audiology and the road ahead: The Army Hearing Program
Mc Ilwain DS et all. Am J Public Health. 2008;98:2167–2172
Il n'y a pas que le PTSD qui soit considéré comme un enjeu majeur de dépistage et de traitement. La perte auditive bénéficie également d'un programme de grande ampleur au sein de l'armée américaine.
Les deux images qui suivent expliquent pourquoi:
1. La fréquence des déficits auditifs liés au combat
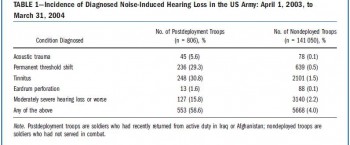
Un point détaillé récent ici
2. L'ouie est un système d'arme:
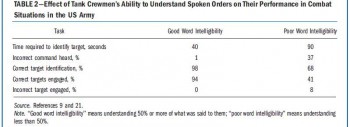
Ce document vous en décrit les grandes lignes
----------------------------------------
" Noise-induced hearing loss has been documented as early as the 16th century, when a French surgeon, Ambroise Pare´ , wrote of the treatment of injuries sustained by firearms and described acoustic trauma in great detail. Even so, the protection of hearing would not be addressed for three more centuries, when the jet engine was invented and resulted in a long overdue whirlwind of policy developmentaddressingtheprevention of hearing loss. We present a synopsis of hearing loss prevention in the US Army and describe the current Army Hearing Program, which aims to prevent noise-induced hearing loss in soldiers and to ensure their maximum combat effectiveness.............
With hearing conservation programs documenting marked initial improvements, the anticipated cost of veterans’ disability claims and payments were expected to decrease over time.10,11 However, with the start of the war in Afghanistan in 2001 and the war in Iraq in 2003, this proved not to be the case. Current data show that 51.8% of combat soldiers have moderately severe hearing loss or worse, mainly because of the loud sounds associated with combat. The implications for the army are great. When soldiers reach these levels of hearing loss, they must be evaluated for the ability to perform their duties safely and effectively. Depending on the findings, they may be given the option of changing to a job that does not put their hearing at further risk or leaving the service with a medical discharge......
."
| Tags : blast
02/11/2013
Blast et audition: Le responsable ?
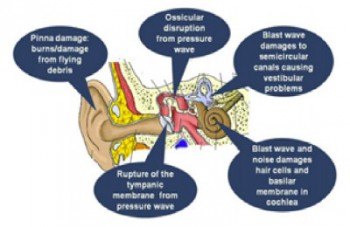
Mechanisms of Hearing Loss after Blast Injury to the Ear
Cho S. et All. Plos One 8(7): e67618. doi:10.1371/journal.pone.0067618
Given the frequent use of improvised explosive devices (IEDs) around the world, the study of traumatic blast injuries is of increasing interest. The ear is the most common organ affected by blast injury because it is the body’s most sensitive pressure transducer. We fabricated a blast chamber to re-create blast profiles similar to that of IEDs and used it to develop a reproducible mouse model to study blast-induced hearing loss. The tympanic membrane was perforated in all mice after blast exposure and found to heal spontaneously. Micro-computed tomography demonstrated no evidence for middle ear or otic capsule injuries; however, the healed tympanic membrane was thickened. Auditory brainstem response and distortion product otoacoustic emission threshold shifts were found to be correlated with blast intensity. As well, these threshold shifts were larger than those found in control mice that underwent surgical perforation of their tympanic membranes, indicating cochlear trauma. Histological studies one week and three months after the blast demonstrated no disruption or damage to the intra-cochlear membranes. However, there was loss of outer hair cells (OHCs) within the basal turn of the cochlea and decreased spiral ganglion neurons (SGNs) and afferent nerve synapses. Using our mouse model that recapitulates human IED exposure, our results identify that the mechanisms underlying blast-induced hearing loss does not include gross membranous rupture as is commonly believed. Instead, there is both OHC and SGN loss that produce auditory dysfunction.
-----------------
Expérimentalement, La perte auditive n'est pas liée à l'atteinte du tympan mais plutôt à l'atteinte des cellules ciliées externes et du ganglion spiral de corti. L'image qui suit tirée d'un autre document vous présente les grandes causes d'atteinte de l'audition.
| Tags : blast
15/10/2013
Dehors et dedans, ce n'est pas la même chose
Primary blast lung injury prevalence and fatal injuries from explosions: Insights from postmortem computed tomographic analysis of 121 improvised explosive device fatalities
SIngleton JAG et all. J Trauma Acute Care Surg. 2013;75: S269-S274.
BACKGROUND:
Primary blast lung injury (PBLI) is an acknowledged cause of death in explosive blast casualties. In contrast to vehicle occupants following an in-vehicle explosion, the injury profile, including PBLI incidence, for mounted personnel following an external explosion has yet to be as well defined.
METHODS:
This retrospective study identified 146 cases of UK military personnel killed by improvised explosive devices (IEDs) between November 2007 and July 2010. With the permission of Her Majesty's Coroners, relevant postmortem computed tomography imaging was analyzed. PBLI was diagnosed by postmortem computed tomography. Injury, demographic, and relevant incident data were collected via the UK Joint Theatre Trauma Registry.
RESULTS:
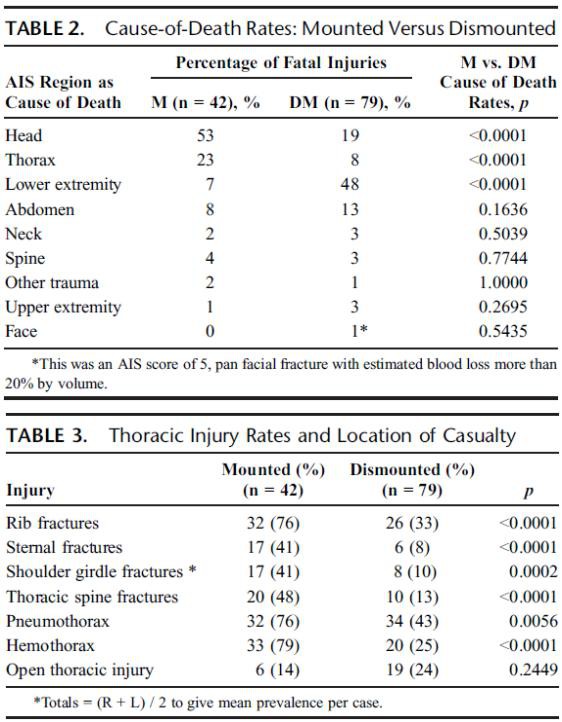
Autopsy results were not available for 1 of 146 cases. Of the remaining 145 IED fatalities, 24 had catastrophic injuries (disruptions), making further study impossible, leaving 121 cases; 79 were dismounted (DM), and 42 were mounted (M). PBLI was noted in 58 cases, 33 (79%) of 42 M fatalities and 25 (32%) of 79 DM fatalities (p < 0.0001). Rates of associated thoracic trauma were also significantly greater in the M group (p < 0.006 for all). Fatal head (53% vs. 23%) and thoracic trauma (23% vs. 8%) were both more common in the M group, while fatal lower extremity trauma (7% vs. 48%) was more commonly seen in DM casualties (p < 0.0001 for all).
CONCLUSION:
Following IED strikes, mounted fatalities are primarily caused by head and chest injuries. Lower extremity trauma is the leading cause of death in dismounted fatalities. Mounted fatalities have a high incidence of PBLI, suggesting significant exposure to primary blast. This has not been reported previously. Further work is required to determine the incidence and clinical significance of this severe lung injury in explosive blast survivors. In addition, specific characteristics of the vehicles should be considered.
| Tags : blast, balistique
21/09/2013
Contamination des plaies: A l'entrée et la sortie
Effect of Initial Projectile Speed on Contamination Distribution in a Lower Extremity Surrogate “Wound Track”
Krebsbach MA et All., Military Medicine, 177, 5:573, 2012
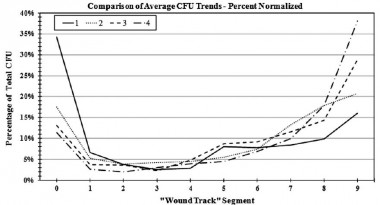
Le nettoyage précoce et la couverture des orifices d'entrée et de sortie sont donc théoriquement des maillons importants de la lutte contre l'infection des plaies de guerre.
| Tags : infection, balistique, pansement
07/09/2013
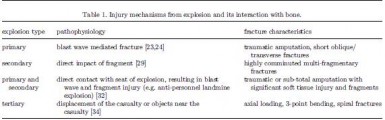
Blast des membres
Blast-related fracture patterns: a forensic biomechanical approach
Ramasamy A. et All. J. R. Soc. Interface (2011) 8, 689–698
Dehors et dedans, ce n'est pas la même chose
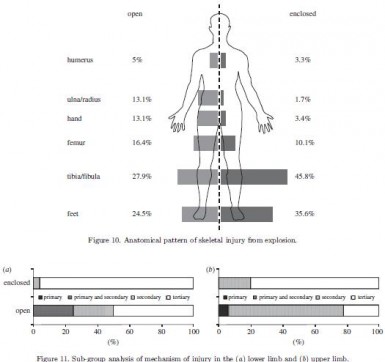
Les lésions dépendent du type de blast
| Tags : blast
25/06/2013
Blast TBI: Un seuil plus bas que pour le poumon
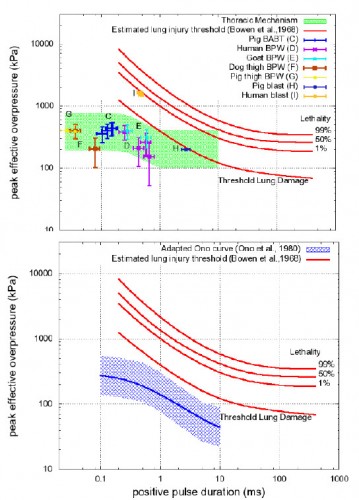
Working toward exposure thresholds for blast-induced traumatic brain injury: thoracic and acceleration mechanisms.
Courtney MW et all. Neuroimage, 2011 Jan,54 Suppl 1: S55-61
Les mécanismes du blast cérébral associent la tansmission de la surpression via le thorax, l'impact direct sur la boite crânienne et les phénomènes d'accélaration de l'extrémité céphalique. Ce document explore la première voie et exprime bien que les seuils lésionnels de lésions cérébrales (courbes de Ono) sont plus bas que les seuils pulmonaires(courbes de Bowden).
| Tags : balistique, tbi
26/03/2013
Mesurer l'exposition au blast: Une réalité
La nécessité de connaître le niveau d'exposition à une onde de blast commence à devenir évidente.Des dispositifs adaptés appraissent sur le marché. Parmi ceux ci le BLAST GAUGE semble intéressant. Porté sur le casque, le gilet pare-balle ou tout autre surface il enregistre l'onde de pression, permet la reconnaissance du niveau par led colorée et l'analyse de la courbe par récupération des données sur un ordinateur.
Le dispositif
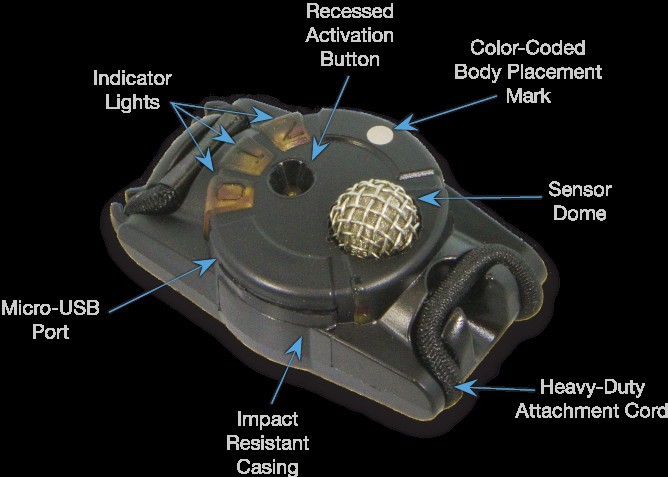
Port sur le casque

D'autres systèmes sont proposés comme le système HEADS de la société BAE dont près de 20 000 dispositfs ont été fournis à l'amée américaine et il est hautement propable que ce type de ce produit va très rapidement être mis en oeuvre dès lors qu'une expsoition à de fortes explosions notamment en milieu clos est attendue.
| Tags : blast, balistique
21/03/2013
Immobilisation du rachis: Dès que possible ! Surtout si VBIED
J Trauma Acute Care Surg. 2013;74: 1112-1118
Si l'atteinte du rachis cervical était dans les derniers conflits est de l'ordre de 1 à 2%, ce taux est monté à 5-8% dans le conflit irakien. Ceci s'explique par l'émergence d'un nouveau mécanisme d'aggression par IED. La procédure du sauvetage au combat stipule que l'imobilisation du rachis cervical ne doit pas être réalisée sous le feu direct de l'ennemi. La frequence des lésions du rachis dans les combats actuels l'impose cependant dès que blessé et sauveteurs sont à l'abri surtout si il s'agit d'un VBIED. C'est que suggère cette publication édifiante qui porte sur l'analyse des lésions du rachis cervical chez les soldats décédés.
| Tags : rachis, balistique
17/02/2013
Ballistic trauma. A practical guide
| Tags : balistique
06/07/2012
Balistique: Actualisation OEF/OIF
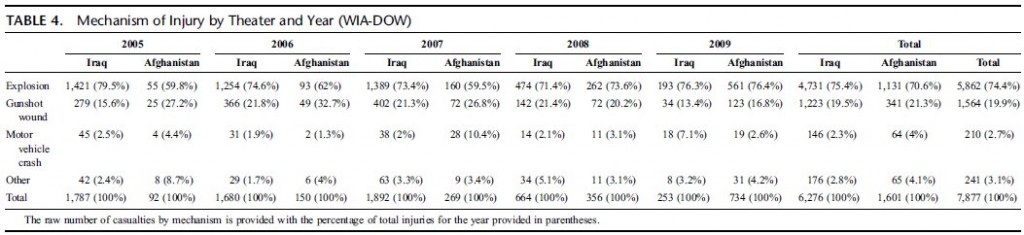
Combat wounds in Iraq and Afghanistan from 2005 to 2009
J Belmont JP et all. (J Trauma Acute Care Surg. 2012;73: 3-12)
Morceaux choisis:
Among the 1,992,232 military service members who were deployed, there were 29,624 distinct combat wounds in 7,877 combat casualties. The mean age of the combat casualty cohort was 26.0 years old. The combat casualties were predominantly male (98I8%), Army (77,5%), and junior enlisted (59,0%). The distribution of combat wounds was as follows: head/neck, 28,1%; thorax, 9,9%; abdomen, 10,1%; and extremities, 51,9%. Explosive injury mechanisms accounted for 74,4% of all combat casualties, which was significantly higher than those caused by gunshot wounds (19,9%) (p G 0.0001). From 2005 to 2007, explosive mechanisms of injury were significantly more common in Iraq than in Afghanistan (p G 0.001). The percentage of explosive mechanisms increased significantly in Afghanistan between the years 2007 (59,5%) and 2008 (73,6%) ( p < 0.0003)
In addition, 1,064 (13,5%) of all combat casualties also sustained burn injuries
| Tags : balistique
03/06/2012
VBIED: Le point UK
In-vehicle extremity injuries from improvised explosive devices: current and future foci
Ramasamy A et all. Phil. Trans. R. Soc. B 2011 366, 160-170
The conflicts in Iraq and Afghanistan have been epitomized by the insurgents’ use of the improvised explosive device against vehicle-borne security forces. These weapons, capable of causing multiple severely injured casualties in a single incident, pose the most prevalent single threat to Coalition troops operating in the region. Improvements in personal protection and medical care have resulted in increasing numbers of casualties surviving with complex lower limb injuries, often leading to long-term disability. Thus, there exists an urgent requirement to investigate and mitigate against the mechanism of extremity injury caused by these devices. This will necessitate an ontological approach, linking molecular, cellular and tissue interaction to physiological dysfunction. This can only be achieved via a collaborative approach between clinicians, natural scientists and engineers, combining physical and numerical modelling tools with clinical data from the battlefield. In this article, we compile existing knowledge on the effects of explosions on skeletal injury, review and critique relevant experimental and computational research related to lower limb injury and damage and propose research foci required to drive the development of future mitigation technologies.

| Tags : balistique