30/09/2015
REBOA: Un savoir faire à maîtriser ?
Implementation of resuscitative endovascular balloon occlusion of the aorta as an alternative to resuscitative thoracotomy for noncompressible truncal hemorrhage
Moor LJ et Al. J Trauma Acute Care Surg. 2015;79: 523-532
L'application du concept du garrot tactique a fait évoluer la répartition des causes évitables de décès à l'avant et met actuellement au premier plan les hémorragies du tronc (Eastridge) . SI le bon usage du garrot reste un enjeu essentiel, les efforts portent maintenant sur la prise en charge d'une part des hémorragies jonctionnelles avec le recours de dispositifs tels que le CRoC, le Sam Junctional tourniquet ou l'abdominal tourniquet et d'autre part sur la prise en charge des hémorragies du tronc. Une autre approche, connue depuis de nombreuses années mais tombée en désuétude, refait surface. L'occlusion endovasculaire de l'aorte abdominale apparaît être d'un intérêt certain. C'est ce que documente le travail présenté ci dessous. Réaliser un tel geste en préhospitalier est possible (1,2). En ce qui concerne les applications militaires dans les structures chirurgicales de role 2 voire dans certaines moyens de transport préhospitalier une réflexion apparaît nécessaire.
------------------------------------------
BACKGROUND:
Hemorrhage remains the leading cause of death in trauma patients. Proximal aortic occlusion, usually performed by direct aortic cross-clamping via thoracotomy, can provide temporary hemodynamic stability, permitting definitive injury repair. Resuscitative endovascular balloon occlusion of the aorta (REBOA) uses a minimally invasive, transfemoral balloon catheter, which is rapidly inserted retrograde and inflated for aortic occlusion, and may control inflow and allow time for hemostasis. We compared resuscitative thoracotomy with aortic cross-clamping (RT) with REBOA in trauma patients in profound hemorrhagic shock.
METHODS: Trauma registry data was used to compare all patients undergoing RTor REBOA during an 18-month period from two Level 1 trauma centers.
RESULTS: There was no difference between RT (n = 72) and REBOA groups (n = 24) in terms of demographics, mechanism of injury, or Injury Severity Scores (ISSs). There was no difference in chest and abdominal Abbreviated Injury Scale (AIS) scores between the groups. However, the RT patients had lower extremity AIS score as compared with REBOA patients (1.5 [0-3] vs. 4 [3-4],p G 0.001). Of the 72 RT patients, 45 (62.5%) died in the emergency department, 6 (8.3%) died in the operating room, and 14 (19.4%) died in the intensive care unit. Of the 24 REBOA patients, 4 (16.6%) died in the emergency department, 3 (12.5%) died in the operating room, and 8 (33.3%) died in the intensive care unit. In comparing location of death between the RT and REBOA groups, there were a significantly higher number of deaths in the emergency department among the RT patients as compared with the REBOA patients (62.5% vs. 16.7%, p G 0.001). REBOA had fewer early deaths and improved overall survival as compared with RT (37.5% vs. 9.7%, p = 0.003).
CONCLUSION: REBOA is feasible and controls noncompressible truncal hemorrhage in trauma patients in profound shock. Patients undergoing REBOA have improved overall survival and fewer early deaths as compared with patients undergoing RT.
| Tags : junctionnel
26/09/2015
La guerre de Crimée: Le rapport de Baudens
Clic sur l'image pour accéder au document
Un écrit où tout est dit. Ce document doit être considéré comme étant fondateur de la médecine de guerre de sa pratique, de son évaluation et de son enseignement. Un vision éminemment moderne et très actuelle. Un écrit majeur par un homme que nous avons oublié.
Petit passage savoureux:
Sur un champ de bataille, la variété et la multiplicité des projectiles, le jeu de la mitraille, produisent à chaque instant un ensemble imprévu de blessures plus affreuses les unes que les autres. Ici plus de règles tracées, tout est à impro viser ; il faut s'ingénier vite et bien pour arrêter la vie, qui s'échappe à travers la plaie. Sur ce théâtre sanglant, il ne suffit pas d'être savant, il faut de plus posséder un coup d'oeil rapide, une intelligence prompte et toujours en éveil. C'est ce génie instinctif, si précieux, si nécessaire, que je voudrais voir développer, à l'école du Val de Grâce, parmi les stagiaires qui doivent peupler, le corps de santé de l'armée.
24/09/2015
Coup de chaleur: Position US
Le coup de chaleur d'exercice est une réalité. Un refroidissement obtenu en moins de 30 minutes est indispensable. L'immersion corps entier est la méthode la plus efficace mais n'est pas forcément disponible. Le refroidissement par immersion des membres supérieurs est discuté. Une approche très intéressante semble être l'emploi de nouvelles couvertures refroidissantes (lien) qui permettent un abaissement significatif des mesures de refroississement dès le lieu de prise en charge et pendant toute la phase de transport.
| Tags : hyperthermie
21/09/2015
Dominique Larrey

20/09/2015
Lucien Jean Baptiste Baudens
Gaspard Léonard Scrive

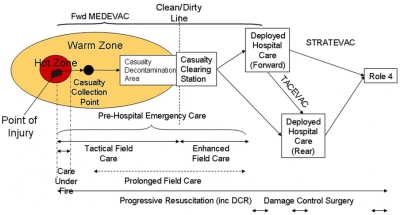
The Operational Patient Care Pathway
The Operational Patient Care Pathway
Une évolution importante de nos amis anglais qui précise le concept du "Prolonged Field Care" et révisent le concept de la golden Hour et des minutes de platine pour le 10-1-2 + 2
For debate: the Operational Patient Care Pathway
Bricknell M. J R Army Med Corps. 2014 Mar;160(1):64-9
| Tags : tactique
18/09/2015
Coagulopathie traumatique: Mécanismes
Trauma-Induced Coagulopathy: An Institution's 35 Year Perspective on Practice and Research
Gonzales E. et Al. Scandinavian Journal of Surgery 103: 89–103, 2014

| Tags : coagulopathie
12/09/2015
Abord trachéal: Point sur l'équipement
Equipment and strategies for emergency tracheal access in the adult patient
Hamaekers AE et Al; Anaesthesia, 2011, 66 (Suppl. 2), pages 65–80
The inability to maintain oxygenation by non-invasive means is one of the most pressing emergencies in anaesthesia and emergency care. To prevent hypoxic brain damage and death in a ‘cannot intubate, cannot oxygenate’ situation, emergency percutaneous airway access must be performed immediately. Even though this emergency is rare, every anaesthetist should be capable of performing an emergency percutaneous airway as the situation may arise unexpectedly. Clear knowledge of the anatomy and the insertion technique, and repeated skill training are essential to ensure completion of this procedure rapidly and successfully. Various techniques have been described for emergency oxygenation and several commercial emergency cricothyroidotomy sets are available. There is, however, no consensus on the best technique or device. As each has its limitations, it is recommended that all anaesthetists are skilled in more than one technique of emergency percutaneous airway. Avoiding delay in initiating rescue techniques is at least as important as choice of device in determining outcome.
| Tags : airway
Ouvrir un cou: Le doigt est important +++
| Tags : coniotomie
01/09/2015
Grimage ou mannequins ? Les 2 svp !
A comparison of live tissue training and high-fidelity patient simulator: A pilot study in battlefield trauma training
Savage EC et Al. J Trauma Acute Care Surg. 2015;00: 00_00[Epub ahead of print].
BACKGROUND:
Trauma procedural and management skills are often learned on live tissue. However, there is increasing pressure to use simulators because their fidelity improves and as ethical concerns increase. We randomized military medical technicians (medics) to training on either simulators or live tissue to learn combat casualty care skills to determine if the choice of modality was associated with differences in skill uptake.
METHODS:
Twenty medics were randomized to trauma training using either simulators or live tissue. Medics were trained to perform five combat casualty care tasks (surgical airway, needle decompression, tourniquet application, wound packing, and intraosseous line insertion). We measured skill uptake using a structured assessment tool. The medics also completed exit questionnaires and interviews to determine which modality they preferred.
RESULTS:
We found no difference between groups trained with live tissue versus simulators in how they completed each combat casualty care skill. However, we did find that the modality of assessment affected the assessment score. Finally, we found that medics preferred trauma training on live tissue because of the fidelity of tissue handling in live tissue models. However, they also felt that training on simulators also provided additional training value.
CONCLUSION:
We found no difference in performance between medics trained on simulators versus live tissue models. Even so, medics preferred live tissue training over simulation. However, more studies are required, and future studies need to address the measurement bias of measuring outcomes in the same model on which the study participants are trained.