31/05/2014
Pansements hémostatiques: Utilité non démontrée
Haemostatic dressings in prehospital care
Hewitt Smith A. et Al. Emerg Med J 2013; 30:784–789
--------------------------------------------------------------
Une revue de littérature qui confirme que le bien fondé de l'emploi des pansements hémostatiques n'est pas si solide que cela. Pansement compressif et packing de plaie sont des valeurs sûres.
--------------------------------------------------------------
| Tags : pansement, hémorragie, massive bleeding control
27/05/2014
Maîtrise de la coniotomie en environnement austère: Une nécessité.
Optimizing Emergent Surgical Cricothyrotomy for use in Austere Environments
HessertMJ et Al. Wilderness Environ Med. 2013 Mar;24(1):53-66
" Although cricothyrotomy is becoming less common as other alternative airway devices are introduced, such as the laryngeal mask airway, King LT-D (King Systems Corp, Noblesville, IN), and other supraglottic devices, there is, and likely always will be, a role for cricothy- rotomy in a subsection of patients with difficult airways, especially in environments in which such devices are unlikely to be available. A common emergency medicine aphorism is: “If you do one cricothyrotomy, you’re a hero; if you do two, work on your airway skills.” True perhaps in a hospital, but in an austere environment many factors besides failed ET intubation lead to early cricothyrotomy. Wilderness providers must be not only technically skilled, but also adequately trained to recognize the key indications and situational decision triggers for cricothyrotomy that differ from in-hospital practice."
| Tags : airway, coniotomie, intubation
26/05/2014
International journal of burns and trauma

Clic sur l'image pour accéder à la revue en ligne
24/05/2014
Gelures: Une vision actualisée 2014
Frostbite: a practical approach to hospital management
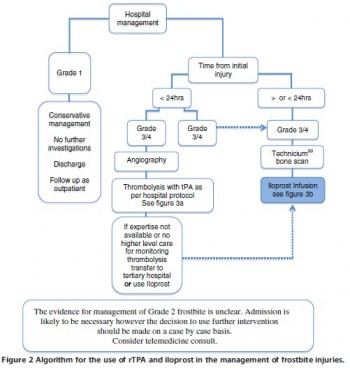
| Tags : gelures
23/05/2014
Manoeuvre de Sellick: Questions/Réponses
Cricoid Pressure in Emergency Department Rapid Sequence Tracheal Intubations: A Risk-Benefit Analysis
Ellis DY et Al. An Emerg Med. 2007 Dec;50(6):653-65
La manœuvre de Sellick est une technique de compression du cartilage cricoïde, décrite en 1961 par Sellick BA. Lors de la réalisation d'une intubation trachéale, elle est utilisée pour prévenir le risque de régurgitation du contenu gastrique et œsophagien vers le pharynx et son inhalation bronchique et alvéolaire lors de l'induction anesthésique qui entraîne une dépression des réflexes de protection des voies aériennes, chez un patient dont l’estomac est plein.
Elle consiste à appuyer fermement sur le cartilage cricoïde qui va alors comprimer l'extrémité supérieure de l'œsophage dont les parois sont souples, contre le corps vertébral de la vertèbre cervicale sous-jacente, rigide. L'intensité de la force à exercer doit être d'environ 20 newtons (N) si le patient est conscient et de 30 N s'il est inconscient2. Cette force est suffisante pour prévenir la régurgitation (inefficace si inférieure à 10 N), n'entraîne pas de sensation nauséeuses susceptibles d'augmenter l'inhalation du contenu gastrique et met à l'abri d'une rupture œsophagienne.
Le taux d'efficacité de la manœuvre de Sellick n'est pas bien établi, techniquement simple, elle est pourtant souvent mal réalisée.
-----------------------------------------------------------------------
Cricoid pressure is considered an integral part of patient safety in rapid sequence tracheal intubation and emergency airway management. Cricoid pressure is applied to prevent the regurgitation of gastric contents into the pharynx and subsequent aspiration into the pulmonary tree. This review analyzes the published evidence supporting cricoid pressure, along with potential problems, including increased difficulty with tracheal intubation and ventilation. According to the evidence available, the universal and continuous application of cricoid pressure during emergency airway management is questioned. An awareness of the benefits and potential problems with technique allows the practitioner to better judge when cricoid pressure should be used and instances in which it should be removed.
-----------------------------------------------------------------------
Le travail présenté répond à un certain nombre d'interrogations et précise pourquoi la réalisation de cette manoeuvre est remise en question.
| Tags : airway
22/05/2014
L'actusanté australien
13/05/2014
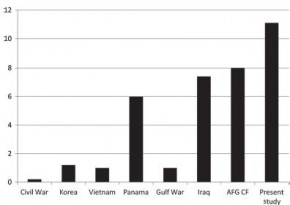
Lésions rachidiennes: Plus fréquentes qu'envisagé
Spinal Injuries in United States Military Personnel Deployed to Iraq and Afghanistan
An Epidemiological Investigation Involving 7877 Combat Casualties From 2005 to 2009
Schoenfeld AJ et All. Spine 2013;38:1770–1778
Les lésions du rachis sont plus fréquentes que ce qui était supposé. Ce travail rapporte qu'une atteinte du rachis est présente dans 11% des cas. Une des explications est que l'amélioration des conditions de prise en charge permet la survie de blessés plus graves qu'auparavant, qui autrefois ne survivait pas à leurs blessures.
-----------------------------------------------------------
In the years 2005 to 2009, 872 (11.1%) casualties with spine injuries were identified among a total of 7877 combat wounded. The mean age of spine casualties was 26.6 years. Spine fractures were the most common injury morphology, comprising 83% of all spinal wounds. The incidence of combat-related spinal trauma was 4.4 per 10,000, whereas that of spine fractures was 4.0 per 10,000. Spinal cord injuries occurred at a rate of 4.0 per 100,000.
Spinal cord injuries were most likely to occur in Afghanistan (incident rate ratio: 1.96; 95% confi dence interval: 1.68–2.28), among Army personnel (incident rate ratio: 16.85; 95% confidence interval: 8.39–33.84), and in the year 2007 (incident rate ratio: 1.90; 95% confi dence interval: 1.55–2.32). Spinal injuries from gunshot were significantly more likely to occur in Iraq (17%) than in Afghanistan (10%, P = 0.02).
-----------------------------------------------------------
| Tags : rachis
Douleur du combattant blessé
La prise en charge de la douleur à l'avant fait appel à l'association de mesures passant par les immobilisations, le recours à la morphine sous cutanée, le paracétamol et dès que possible certaines techniques d' ALR. Les US viennent de proposer l'évolution de leur vision des choses.
Clic sur l'image pour accéder au document