18/10/2017
On peut rêver

Philippe Chapleau nous apprend que dans le cadre de son déploiement en Europe, les 1900 soldats de la 1st Air Cavalry Brigade disposera disposeront de 12 Chinook, 38 Black Hawk, 24 Apache et 15 Black Hawk médicalisés. On peut rêver.
| Tags : medevac
26/03/2017
MEDEVAC Sangaris: Du médical avant tout
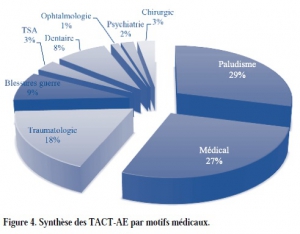
Évacuations médicales aériennes tactiques et stratégiques en République centrafricaine au cours de l’opération « Sangaris ». Synthèse des onze premiers mois d’opérations
Beylot V. et Al. médecine et armées, 2016, 44, 4, 087-096
-------------------------------------
Un état des lieux intéressants qui n'est pas sans rappeler l'histoire de nos anciens confrontés à l'isolement et à la dureté du climat. Les causes médicales de MEDEVAC en première ligne dont le Paludisme ?, les envenimations scorpioniques, les problèmes dentaires. Les blessures par armes de guerre apparaissent beaucoup moins fréquentes. Le contexte d'intervention: une guerre civile, les élongations et les problèmes climatiques expliquent beaucoup de chose. Une grosse différence l'emploi quasi systématique, hors Bangui, du vecteur aérien pour les medevac, vecteur ldont la mise en oeuvre a pu être optimisé par un centre de coordination dont le rôle est essentiel.
-------------------------------------
Au cours des onze premiers mois de l’opération « Sangaris », 249 évacuations médicales aériennes tactiques et 186 évacuations médicales aériennes stratégiques ont été réalisées. Nous proposons ici une présentation synthétique de ces évacuations. Dans les motifs d’évacuation, la place importante du paludisme (29 % des évacuations tactiques) est un reflet de l’épidémie à laquelle les forces françaises ont été confrontées. Les conditions de déploiement en interposition ont pu amplifier l’impact psychiatrique de cette mission (28 % des évacuations stratégiques) et participer à la réouverture du sas de fin de mission. La place des blessures de guerres (9 % des évacuations tactiques et 13 % des évacuations stratégiques) majoritairement dues à des éclats de grenades reste importante et illustre le risque inhérent à cet engagement.
Enfin, si la chaîne de santé complète déployée au plus proche, en passant notamment par la nomadisation des équipes héliportées, a permis d’assurer un soutien médical de qualité, l’étendue de ce théâtre nous interpelle sur les délais et la catégorisation utilisée lors des évacuations tactiques.
| Tags : medevac
03/12/2016
Combat MEDEVAC: Par qui ?
Combat MEDEVAC: A comparison of care by provider type for en route trauma care in theater and 30-day patient outcomes.
---------------------------------------------
L'intérêt e la présence d'un personnel à bord d'un vecteur d'évacuation est l'objet de débats passionnés. Le travail présenté ici rapporte l'analyse de MEDEVAC conduites sur le territoire afghan par nos alliés américains. Il ne met pas en évidence d'apport significatif d'équipes disposant de pratiques avancés en traumatologie, y compris pour les blessés les plus sévères. Il confirme le nombre limité de procédures mises en oeuvre (1). Il met même en évidence le moindre recours à des pratiques transfusionnelles dans ce groupe de personnels par rapport au groupe Paramedic, alors que plus d'abord vasculaire et d'apport de liquide de remplissage est conduit. On peut légitimement s'étonner de ces résultats car d'autres publications mettent en avant l'apport de la présence de praticiens disposant de connaissances avancées dans ce domaine (2). la composition de ce groupe de personnels aux pratiques avancées interpelle quand même car il contient des infirmiers des médecins et des assistants médecins dont l'expertise réelle en matière de prise en charge de traumatisés reste non décrite. On peut se poser la question d'une expertise moindre que celle des Paramedics dont le cursus de formation est d'excellente qualité (3). Une autre explication peut être trouvée par la spécificité du territoire afghan où les temps de transport étaient au final assez brefs, sans commune mesure avec celui d'autres théâtres d'intervention, notamment africains (4). Les conditions actuelles de soutien médical nous montre bien que la mise en oeuvre de pratiques avancées par du personnel non seulement PRATIQUANT mais aussi EXPERT doit rester l'objectif essentiel. Un vrai challenge pour les années à venir.
BACKGROUND:
Medical evacuation (MEDEVAC) is the movement and en route care of injured and medically compromised patients by medical care providers via helicopter. Military MEDEVAC platforms provide lifesaving interventions that improve survival in combat. There is limited evidence to support decision making related to en route care and allocation of resources. The association between provider type and en route care is not well understood. Our objective was to describe MEDEVAC providers and identify associations between provider type, procedures performed, and outcomes.
METHODS:
We conducted an institutional review board-approved, retrospective record review of patients traumatically injured incombat, evacuated by MEDEVAC from the point of injury, between 2011 and 2014. Data abstracted included injury description, provider type, procedures performed, medications administered, survival, and 30-day outcomes. Subjects were grouped according to provider type: medics, paramedics, and ADVs (advanced-level providers to include nurses, physician assistants, and physicians). Groups were compared. Analyses were performed using χ tests for categorical variables and analysis of variance tests (Kruskal-Wallis tests) for continuous variables; p < 0.05 was considered significant.
RESULTS:
The MEDEVAC records were reviewed, and data were abstracted from 1,237 subjects. The providers were composed of medics, 76%; paramedics, 21%; and ADVs, 4%. Patient and injury demographics were similar among groups. The ADVs were most likely to perform intubation, chest needle decompressions (p < 0.0001), and hypothermia prevention (p = 0.01). Paramedics were most likely to administer blood en route (p < 0.0001). All other procedures were similar between groups. Paramedics were most likely to administer ketamine (p < 0.0001), any analgesic (p < 0.0001), or any medication en route (p < 0.0001). Incidence rates of en route events (pain, hypoxia, abnormal hemodynamics, vital signs) were similar between provider types. In-theater and 30-day survival rates were similar between provider types.
CONCLUSION:.
Providers with higher-level training were more likely to perform more advanced procedures during en route care. .y found no.ficant .ociati. bet.ee. More evidence is needed to determine the appropriate level of MEDEVAC personnel training and skill maintenance necessary to minimize combat mortality.
| Tags : medevac
24/09/2016
MEDEVAC: Une réanimation avancée rapporte
A review of the first 10 years of critical care aeromedical transport during operation iraqi freedom and operation enduring freedom: the importance of evacuation timing
Ingals N et Al. JAMA Surg. 2014 Aug;149(8):807-13
------------------------------------------
Ce document est très intéressant car il met en avant l'intérêt du transport des blessés de guerre par des équipes maîtrisant toutes les facettes du damage control resusictation tant au niveau médical que paramédical. Une approche très similaire est celle des MERT-E
------------------------------------------
Advances in the care of the injured patient are perhaps the only benefit of military conflict. One of the unique aspects of the military medical care system that emerged during Operation Iraqi Freedom and Operation Enduring Freedom has been the opportunity to apply existing civilian trauma system standards to the provision of combat casualty care across an evolving theater ofoperations.
OBJECTIVES:
To identify differences in mortality for soldiers undergoing early and rapid evacuation from the combat theater and to evaluate the capabilities of the Critical Care Air Transport Team (CCATT) and Joint Theater Trauma Registry databases to provide adequate data to support future initiatives for improvement of performance.
DESIGN, SETTING, AND PARTICIPANTS:
Retrospective review of CCATT records and the Joint Theater Trauma Registry from September 11, 2001, to December 31, 2010, for the in-theater military medicine health system, including centers in Iraq, Afghanistan, and Germany. Of 2899 CCATT transport records, those for 975 individuals had all the required data elements.
EXPOSURE:
Rapid evacuation by the CCATT.
MAIN OUTCOMES AND MEASURES:
Survival as a function of time from injury to arrival at the role IV facility at Landstuhl Regional Medical Center.
RESULTS:
The patient cohort demonstrated a mean Injury Severity Score of 23.7 and an overall 30-day mortality of 2.1%. Mortality en route was less than 0.02%. Statistically significant differences between survivors and decedents with respect to the Injury Severity Score (mean [SD], 23.4 [12.4] vs 37.7 [16.5]; P < .001), cumulative volume of blood transfused among the patients in each group who received a transfusion (P < .001), worst base deficit (mean [SD], -3.4 [5.0] vs -7.8 [6.9]; P = .02), and worst international normalized ratio (median [interquartile range], 1.2 [1.0-1.4] vs 1.4 [1.1-2.2]; P = .03) were observed. We found no statistically significant difference between survivors and decedents with respect to time from injury to arrival at definitive care.
CONCLUSIONS AND RELEVANCE:
Rapid movement of critically injured casualties within hours of wounding appears to be effective, with a minimal mortality incurred during movement and overall 30-day mortality. We found no association between the duration of time from wounding to arrival at Landstuhl Regional Medical Center with respect to mortality.
| Tags : medevac
21/10/2015
Conditionner un blessé grave

Clic sur l'image pour accéder au document
| Tags : medevac
21/06/2015
Un nouveau concept de triage ?
Medical evacuation and triage of combat casualties in Helmand Province, Afghanistan: October 2010-April 2011
Clarke JE et Al. Mil Med. 2012 Nov;177(11):1261-6
--------------------------------------------------------------------
Un article de synthèse sur l'organisation de la chaîne de prise en charge des blessés par nos confrères anglais, avec notamment l'emploi d'une évolution majeure pour le un système anglo-saxon (lire ce document): le recours à des EVASAN médicalisées par des personnels ayant une pratique régulière de la prise en charge de patients en état critique. Cet article est intéressant car il insiste sur l'importance du triage et le rôe prééminent que peuvent jouer les role 2 notamment si les élongations sont importantes.
--------------------------------------------------------------------
Medical evacuation of combat casualties in Operation Enduring Freedom-Afghanistan is achieved primarily by helicopter, because of distances involved as well as ground-based threats. In Helmand Province, evacuation from the point of injury may occur on a variety of helicopter evacuation platforms with disparate levels of attendant medical expertise. Furthermore, triage to a medical treatment facility may involve varying echelons of care before definitive management. Consequently, considerable differences in medical care may be encountered between point of injury and definitive treatment. We discuss the role of helicopter-based medical evacuation in Helmand, Afghanistan, as well as triage and timelines to the most appropriate medical facilities. Based on our experience and available evidence, we have made recommendations to regional commanders which favor the utilization of prehospital critical care teams aboard helicopter-based evacuation platforms and direct triage to the highest echelon of care available when feasible
Médecin EXPERIMENTÉ: Pronostic amélioré
Determining the composition and benefit of the pre-hospital medical response team in the conflict setting
Davis PR et Al. J R Army Med Corps. 2007 Dec;153(4):269-73
----------------------------------------------------------------
La composition des équipes d'evasan tactique fait débat. La présence d'un médecin serait associée à une meilleure survie des blessés les plus graves, surtout si les délais de prise en charge par une équipe chirurgicales sont longs. Encore faut il que ce médecin ait de réelles compétences en matière de traumatologie et d'exercice de la médecine préhospitalière en situation isolée.
----------------------------------------------------------------
Aim: To determine the optimal composition of the pre-hospital medical response team (MERT) and the value of prehospitalvcritical care interventions in a military setting, and specifically to determine both the benefit of including a doctor in the pre-hospital response team and the relevance of the time and distance to definitive care.
Method: A comprehensive review of the literature incorporating a range of electronic search engines and hand searches of key journals.
Results: There was no level 1 evidence on which to base conclusions. The 15 most relevant articles were analysed in detail. There was one randomized controlled trial (level 2 evidence) that supports the inclusion of a doctor on MERT. Several cohort studies were identified that analysed the benefits of specific critical care interventions in the pre-hospital setting.
Conclusions: A doctor with critical care skills deployed on the MERT is associated with improved survival in victims of major trauma. Specific critical care interventions including emergency endotracheal intubation and ventilation, and intercostal drainage are associated with improved survival and functional recovery in certain patients.
16/06/2015
Doctors on board, utile ?
Doctor on board? What is the optimal skill-mix in military pre-hospital care?
Calderbank P et Al. Emerg Med J. 2011 Oct;28(10):882-3
-----------------------------------------------------
Le recul des MERT-E anglaise dans un contexte bien particulier où le temps de vol moyen est de 3/4 d'heure. La présence d'un médecin n'est pas déterminante. Ce n'est pas du tout la même chose si les temps de vol sont longs (1).
-----------------------------------------------------
BACKGROUNDS: In a military setting, pre-hospital times may be extended due to geographical or operational issues. Helicopter casevac enables patients to be transported expediently across all terrains. The skill-mix of the pre-hospital team can vary.
AIM: To quantify the doctors' contribution to the Medical Emergency Response Team-Enhanced (MERT-E).
METHODS: A prospective log of missions recorded urgency category, patient nationality, mechanism of injury, medical interventions and whether, in the crew's opinion, the presence of the doctor made a positive contribution.
RESULTS: Between July and November 2008, MERT-E flew 324 missions for 429 patients. 56% of patients carried were local nationals, 35% were UK forces. 22% of patients were T1, 52% were T2, 21.5% were T3 and 4% were dead. 48% patients had blast injuries, 25% had gunshot wounds, 6 patients had been exposed to blast and gunshot wounds. Median time from take-off to ED arrival was 44 min. A doctor flew on 88% of missions. It was thought that a doctor's presence was not clinically beneficial in 77% of missions. There were 62 recorded physician's
INTERVENTIONS: The most common intervention was rapid sequence induction (45%); other interventions included provision of analgesia, sedation or blood products (34%), chest drain or thoracostomy (5%), and pronouncing life extinct (6%).
CONCLUSION: MERT-E is a high value asset which makes an important contribution to patient care. A relatively small proportion of missions require interventions beyond the capability of well-trained military paramedics; the indirect benefits of a physician are more difficult to quantify.
| Tags : medevac
10/03/2015
Thèse Medevac Africaines
| Tags : medevac