22/02/2018
Penthrox ?: Franchement pas une nouveauté
A review of the safety and efficacy of inhaled methoxyflurane as an analgesic for outpatient procedures
C. Jephcott et Al. British Journal of Anaesthesia, ▪ (▪): 1e9 (2018)
------------------------------------------
Le méthoxyflurane (Penthrox) est un agent d'anesthésie halogéné, connu depuis les années 50 et tombé en désuétude à cause essentiellement de sa néphrotoxicité importante. Il semble être remis au goût du jour et est actuellement proposé pour des propriétés antalgiques qu'il partage avec tous les agents de sa classe pharmaceutique. Si son principe d'emploi apparaît intéressant, il existe des limites à son intérêt: Une technique d'inhalation à bien maîtriser, quelques effets secondaires notamment hypotension et somnolence, pas plus de 15 ml par semaine. Si son emploi sur de courtes durées permet de limiter le risque rénal, le risque d'hyperthermie maligne peranesthésique est toujours présent. Son efficacité serait équivalente à celle du meopa (1) et pour certains légèrement inférieure à celle de la morphine (2). La Commission de la transparence considère que la spécialité PENTHROX n’apporte pas d’amélioration du service médical rendu considéré comme modéré par rapport aux autres antalgiques disponibles (3) notamment pour les douleurs d'origine traumatique. Un médicament ancien remis au goût du jour mais qui cherche son positionnement (4). Son apport reste très discutable tout particulièrement sur les douleurs très sévères (à EVA >7).
------------------------------------------
Methoxyflurane delivered via a hand-held inhaler is a proven analgesic which has been used in Australasia for emergency relief of trauma associated pain since the 1970s. The agent is self-administered by the patient under the supervision of trained personnel. More than 5 million patients have received inhaled methoxyflurane without significant side effects. Methoxyflurane is also licensed in Australasia for the relief of pain in monitored conscious patients requiring analgesia for minor surgical procedures. Recent clinical studies undertaken in a variety of outpatient settings, including colonoscopy, prostate biopsy, dental procedures, bone marrow biopsy, and the management of burns dressings, indicate that inhaled methoxyflurane has significant analgesic activity, without producing deep sedation or respiratory depression. Return to full psychomotor activity is rapid. Thus, methoxyflurane may be a suitable and well-tolerated alternative to traditional i.v. sedative agents for outpatient medical and surgical procedures. There are direct advantages to the patient in terms of rapid recovery and an early return to normal activities, and significant benefits for outpatient departments in terms of cost saving and rate of throughput. Further randomised controlled trials comparing the efficacy, safety, and cost-effectiveness of inhaled methoxyflurane against traditional i.v. sedative techniques are currently in progress.
11/02/2018
Airway: Prévention des complications
Clic sur 'image pour accéder au document
| Tags : airway
06/02/2018
Gilet de protection: A porter près du corps
Do air-gaps behind soft body armour affect protection?
INTRODUCTION:
Body armour typically comprises a fabric garment covering the torso combined with hard armour (ceramic/composite). Some users wear only soft armour which provides protection from sharp weapons and pistol ammunition. It is usually recommended that body armour is worn against the body with no air-gaps being present between the wearer and the armour. However, air-gaps can occur in certain situations such as females around the breasts, in badly fitting armour and where manufacturers have incorporated an air-gap claiming improvements in thermophysiological burden. The effect of an air-gap on the ballistic protection and the back face signature (BFS) as a result of a non-perforating ballistic impact was determined.
METHODS:
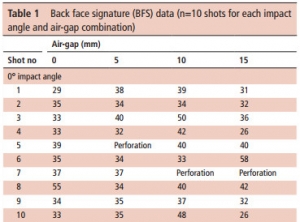
Armour panels representative of typical police armour (400x400 mm) were mounted on calibrated Roma Plastilina No 1 and impacted with 9 mm Luger FMJ (9×19 mm; full metal jacket; Dynamit Nobel DM11A1B2) ammunition at 365±10 m/s with a range of air-gaps(0-15 mm). Whether or not the ammunition perforated the armour was noted, the BFS was measured and the incidence of pencilling (a severe, deep and narrow BFS) was identified.
RESULTS:
For 0° impacts, a critical air-gap size of 10 mm is detrimental to armour performance for the armour/ammunition combination assessed in this work. Specifically, the incidences of pencilling were more common with a 10 mm air-gap and resulted in BFS depth:volume ratios ≥1.0. For impacts at 30° the armour was susceptible to perforation irrespective of air-gap.
CONCLUSIONS:
This work suggested that an air-gap behind police body armour might result in an increased likelihood of injury. It is recommended that body armour is worn with no air-gap underneath.