30/01/2018
Golden hour: Un concept + qu'une obligation

Clic sur l'image pour accéder au document
Un titre accrocheur pour une revue historique et conceptuelle de la médecine tactique. Un plaidoyer pour la conservation d'un minimum d'agilité dans les démarches actuelles
20/01/2018
Queensland Clinical Practice Manual

Clic sur l'image pour accéder aux protocoles
17/01/2018
Guide de médecine rurale AUS
Clic sur l'image pour accéder au document
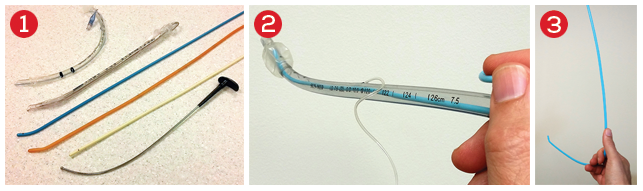
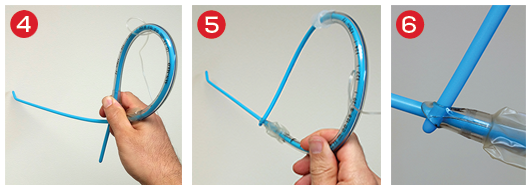
Histoire de mandrin
Il n'est parfois pas simple de bien maintenir un mandrin d'intubation dans le bon axe. Vous sont proposé en 3,4 et 5 plusieurs manières de s'en sortir.
15/01/2018
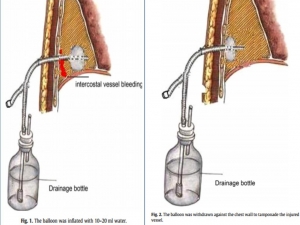
Une sonde de Foley dans le thorax
Balloon Foley catheter compression as a treatment for intercostal vessel bleeding
Chao BF et Al. Injury. 2011 Sep;42(9):958-9.
Avoir DEUX FOLEY avec soi, et ce n'est pas pour faire un sondage urinaire mais pour réaliser un tamponnement nasal, intercostale, d'une plaie cervicale ou tout simpment pour draîner un thorax
09/01/2018
A lire
Prolonged Field Care of a Casualty With Penetrating Chest Trauma Case Report
Barnhart G. et Al. J Spec Oper Med. Winter 2016;16(4):99-101
As Special Operations mission sets shift to regions with less coalition medical infrastructure, the need for quality long-term field care has increased. More and more, Special Operations Medics will be expected to maintain casualties in the field well past the "golden hour" with limited resources and other tactical limitations. This case report describes an extended-care scenario (>12 hours) of a casualty with a chest wound, from point of injury to eventual casualty evacuation and hand off at a Role II facility. This case demonstrates the importance of long-term tactical medical considerations and the effectiveness of minimal fluid resuscitation in treating penetrating thoracic trauma.
Histoire à lire
A Case of Prehospital Traumatic Arrest in a US Special Operations Soldier: Care From Point of Injury to Full Recovery
During an assault on an extremely remote target, a US Special Operations Soldier sustained multiple gunshot and fragmentation wounds to the thorax, resulting in a traumatic arrest and subsequent survival. His care, including care under fire, tactical field care, tactical evacuation care, and Role III, IV, and V care, is presented. The case is used to illustrate the complex dynamics of Special Operations care on the modern battlefield and the exceptional outcomes possible when evidence-based medicine is taken to the warfighter with effective,
03/01/2018
Fibrinogène: En 1er chez les canadiens
Fibrinogen Concentrate in the Special Operations Forces Environment
Sanders S et al. Military Medecine, 00, 0/0:1, 2017
------------------------------------
Un choix raisonné et différent (Apport de 6 g de fibrinogène) des armées françaises qui s'intègre dans les nouvelles stratrégies transfusionnelles de prise en charge du blessé de guerre où la place de la transfusion de sang frais le fibrinogène et le plasma ont une place essentielle (1,2)
Aller sur le forum coagulopathie
------------------------------------
Introduction:
Hemorrhage is the most common cause of death among Special Operations Force (SOF) soldiers. Bringing remote damage control resuscitation into the far-forward combat environment is logistically challenging, as it requires blood products that generally require a robust cold chain. Alternatively, lyophilized products such as fibrinogen concentrate, which does not require thawing or blood group compatibility testing before use, might be advantageous in damage control resuscitation in the battlefield. In this report, we review the evidence for the use of fibrinogen concentrate in the Canadian SOF environment.
Materials and Methods:
The literature on the use of fibrinogen concentrate in the trauma setting was reviewed by Canadian Forces Services Working Group, in three separate meetings. Multiple stakeholders were consulted to obtain authoritative perspectives from subject matter experts on the use of fibrinogen concentrate in the Canadian SOF environment.
We also conducted a comparison review of fibrinogen content, pathogen risk, shelf life, and methods required for use for fresh frozen plasma, cryoprecipitate, and fibrinogen concentrate relevant to their application in the far-forward combat environment.
Results:
Indications and a protocol for the use of fibrinogen as an adjunct to fresh whole blood were formulated based on a literature review and clinical expert opinion. Alternative strategies and other lyophilized blood products were considered before selecting fibrinogen concentrate as the lyophilized blood product of choice. Fibrinogen concentrate is an ABO-universal blood product with an excellent safety profile. Training was conducted by subject matter experts within civilian trauma centers and at military training facilities. The clinical efficacy and safety were confirmed by monitoring the use of fibrinogen concentrate in deployed combat settings.
Conclusion:
Fibrinogen concentrate is a useful adjunct to remote damage control resuscitation in the SOF environment. Fibrinogen concentrate was found to be robust for transport into the SOF environment and is widely accepted among SOF operators and medics
02/01/2018
Immobilisation cervicale: Pas bon !
Prehospital Spine Immobilization/Spinal Motion Restriction in Penetrating Trauma: a Practice Management Guideline from the Eastern Association for the Surgery of Trauma (EAST)
J Trauma Acute Care Surg. 2017 Dec 28
BACKGROUND:
Spine immobilization in trauma has remained an integral part of most emergency medical services (EMS) protocols despite a lack of evidence for efficacy and concern for associated complications, especially in penetrating trauma patients. We reviewed the published evidence on the topic of prehospital spine immobilization or spinal motion restriction in adult patients with penetrating trauma to structure a Practice Management Guideline.
METHODS:
We conducted a Cochrane style systematic review and meta-analysis, and applied GRADE methodology to construct recommendations. Qualitative and quantitative analyses were used to evaluate the literature on the critical outcomes of mortality, neurologic deficit, and potentially reversible neurologic deficit.
RESULTS:
A total of 24 studies met inclusion criteria, with qualitative review conducted for all studies. We used five studies for the quantitative review (meta-analysis). No study showed benefit to spine immobilization with regard to mortality and neurologic injury, even for patients with direct neck injury. Increased mortality was associated with spine immobilization, with RR 2.4 (CI 1.07, 5.41). The rate of neurologic injury or potentially reversible injury was very low, ranging from 0.002 to 0.076 and 0.00034 to 0.055, with no statistically significant difference for neurologic deficit or potentially reversible deficit, RR 4.16 (CI 0.56, 30.89), and RR 1.19 (CI 0.83, 1.70), although the point estimates favored no immobilization.
CONCLUSIONS:
Spine immobilization in penetrating trauma is associated with increased mortality and has not been shown to have a beneficial effect on mitigating neurologic deficits, even potentially reversible neurologic deficits. We recommend that spine immobilization not be used routinely for adult patients with penetrating trauma.