18/03/2018
Combat en montagne: Soutien médical
Challenges of Military Health Service Support in Mountain Warfare
Raimund Lechner et Al. https://doi.org/10.1016/j.wem.2018.01.006
------------------
Un environnement hostile pour des blessés particuliers et des équipes médicales dont l'entraînement doit être au plus haut. Lire aussi
------------------
Introduction
History is full of examples of the influence of the mountain environment on warfare. The aim of this article is to identify the main environmental hazards and summarize countermeasures to mitigate the impact of this unique environment.
Methods
A selective PubMed and Internet search was conducted. Additionally, we searched bibliographies for useful supplemental literature and included the recommendations of the leading mountain medicine and wilderness medicine societies.
Results
A definition of mountain warfare mainly derived from environmental influences on body functions is introduced to help identify the main environmental hazards. Cold, rugged terrain, hypoxic exposure, and often a combination and mutual aggravation of these factors are the most important environmental factors of mountain environment. Underestimating this environmental influence has decreased combat strength and caused thousands of casualties during past conflicts. Some marked differences between military and civilian mountaineering further complicate mission planning and operational sustainability.
Conclusions
To overcome the restrictions of mountain environments, proper planning and preparation, including sustained mountain mobility training, in-depth mountain medicine training with a special emphasize on prolonged field care, knowledge of acclimatization strategies, adapted time calculations, mountain-specific equipment, air rescue strategies and makeshift evacuation strategies, and thorough personnel selection, are vital to guarantee the best possible medical support. The specifics of managing risks in mountain environments are also critical for civilian rescue missions and humanitarian aid.
Control Cric: Pas mieux que la conio chirurgicale
A randomized cross-over study comparing surgical cricothyrotomy techniques by combat medics using a synthetic cadaver model
Cricothyrotomy is a complex procedure with a high rate of complications including failure to cannulate and injury to adjacent anatomy. The Control-Cric™ System and QuickTrach II™ represent two novel devices designed to optimize success and minimize complications with this procedure. This study compares these two devices against a standard open surgical technique.
METHODS:
We conducted a randomized crossover study of United States Army combat medics using a synthetic cadaver model. Participants performed a surgical cricothyrotomy using the standard open surgical technique, Control-Cric™ System, and QuickTrach II™ device in a random order. The primary outcome was time to successful cannulation. The secondary outcome was first-attempt success. We also surveyed participants after performing the procedures as to their preferences.
RESULTS:
Of 70 enrolled subjects, 65 completed all study procedures. Of those that successfully cannulated, the mean times to cannulation were comparable for all three methods: standard 51.0s (95% CI 45.2-56.8), QuickTrach II™ 39.8s (95% CI 31.4-48.2) and the Cric-Control™ 53.6 (95% CI 45.7-61.4). Cannulation failure rates were not significantly different: standard 6.2%, QuickTrach II™ 13.9%, Cric-Control™ 18.5% (p=0.106). First pass success rates were also similar (93.4%, 91.1%, 88.7%, respectively, p=0.670). Of respondents completing the post-study survey, a majority (52.3%) preferred the QuickTrach II™ device.
CONCLUSIONS:
We identified no significant differences between the three cricothyrotomy techniques with regards to time to successful cannulation or first-pass success.
| Tags : airway
12/03/2018
Voies aériennes: L'expérience US OIF/OEF
BACKGROUND:
Airway management is of critical importance in combat trauma patients. Airway compromise is the second leading cause of potentially survivable death on the battlefield and accounts for approximately 1 in 10 preventable deaths. Reports from the Iraq and Afghanistan wars indicate 4-7% incidence of airway interventions on casualties transported to combat hospitals. The goal of this study was to describe airway management in the prehospital combat setting and document airway devices used on the battlefield.
METHODS:
This study is a retrospective review of casualties that required a prehospital life-saving airway intervention during combat operations in Afghanistan. We obtained data from the Prehospital Trauma Registry (PHTR) that was linked to the Department of Defense Trauma Registry (DoDTR) for outcome data for the time period between January 2013 and September 2014.
RESULTS:
705 total trauma patients were included, 16.9% required a prehospital airway management procedure. There were 132 total airway procedures performed, including 83 (63.4%) endotracheal intubations and 26 (19.8%) nasopharyngeal airway placements. Combat medics were involved in 48 (36.4%) of airway cases and medical officers in 73 (55.3%). Most (94.2%) patients underwent airway procedures due to battle injuries caused by explosion or gunshot wounds.
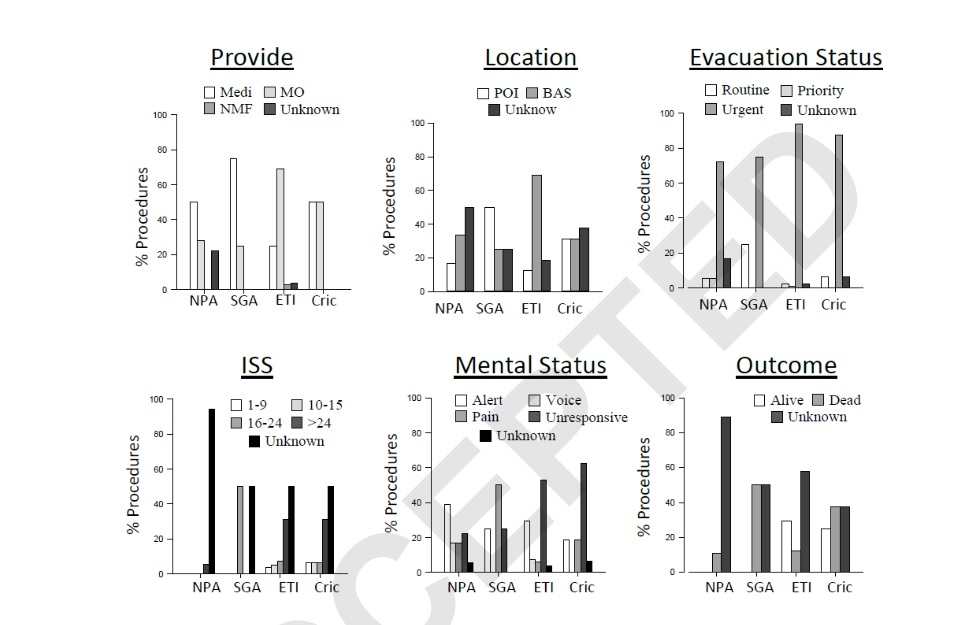
Casualties requiring airway management were more severely injured and less likely to survive as indicated by injury severity score, responsiveness level, Glascow coma score, and outcome.
CONCLUSIONS:
Percentages of airway interventions more than tripled from previous reports from the wars in Afghanistan and Iraq. These changes are significant and further study is needed to determine the causes. Casualties requiring airway interventions sustained more severe injuries and experienced lower survival than patients who did not undergo an airway procedure, findings suggested in previous reports.
01/03/2018
Trauma jonctionnels: Une revue
Clic sur l'image pour accéder au document
| Tags : jonctionnel, hémorragie