20/12/2013
Drainage et thoracocentèse
Chest Drainage
McDermott S. et Al. Semin Intervent Radiol 2012;29:247–255
Infectious, traumatic, or neoplastic processes in the chest often result in fluid collections within the pleural, parenchymal, or mediastinal spaces. The same fundamental principles that guide drainages of the abdomen can be applied to the chest. This review discusses various pathologic conditions of the thorax that can result in the abnormal accumulation of fluid or air, and their management using image-guided methods.
16/12/2013
Gelures: Le guidelines de la WMS
| Tags : gelures
15/12/2013
Portoir d'extraction de blessés
L'extraction de blessé par des moyens de portage léger est une gageure. Certains filets sont utiles mais de préhension difficile sur de longues distances. Il existe des équivalents en toile pleine plus ou moins épaisse qui peuvent représenter une solution. Le produit présenté ici est un produit DIMATEX, évolution du filet golanis et du spad, qui a pour originalité de pouvoir servir en outre de hamac, d'abri de fortune (on peut associer deux portoirs grâce à un système de velchro: on retrouve là le principe des anciennes tentes individuelles), de coupe-vent (intérêt dans la prévention de l'hypothermie), voire de protège-pluie. Un système de sangle permet la traction même si de par sa conception il n'est pas prévu pour traîner un blessé au sol.
A priori un très bon compromis taille/Encombrement/poids fonctionnalité

| Tags : brancardage, extraction
14/12/2013
Paludisme

Le paludisme est une maladie provoquée par des parasites du genrePlasmodium. Selon l’OMS, cette maladie cause aux alentours d’1 million de victimes par an dans le monde. Environ 40% de la population mondiale est exposée à la maladie et 500 millions de cas cliniques sont observés chaque année. La situation est d’autant plus préoccupante que depuis plusieurs années les parasites développent des résistances aux molécules antipaludiques et les moustiques craignent de moins en moins les insecticides. Aujourd’hui, aucun vaccin n’est disponible. (la fiche de l'institut Pasteur)
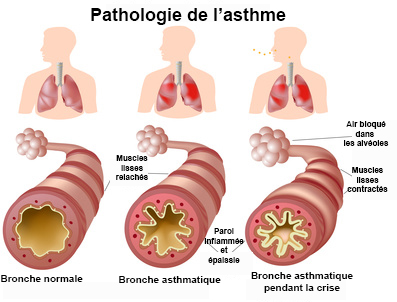
Asthme aigu grave
La rage

La rage reste une maladie très répandue dans le monde, responsable de dizaines de milliers de morts chaque année. Elle est le plus souvent transmise par les chiens. En Europe, les chauves-souris, qui hébergent des virus différents de ceux du chien ou du renard, sont particulièrement surveillées. La maladie est mortelle en l’absence de traitement. (la fiche de l'institut Pasteur)
Le choléra

Le choléra est une maladie diarrhéique épidémique, strictement humaine, due à des bactéries appartenant aux sérogroupes O1 et O139 de l’espèce Vibrio cholerae. Ce bacille fût initialement observé par Pacini en 1854 puis isolé en 1883 par Koch en Egypte. La bactérie Vibrio cholerae sérogroupe O1, biotype El Tor, est répandue sur toute la planète, qui subit actuellement la septième pandémie de choléra. En 2009, 221 226 cas dont 4946 mortels, ont été déclarés à l’Organisation Mondiale de la Santé par 45 pays, appartenant à tous les continents à l’exception de l’Amérique centrale et de l’Amérique du Sud. L’Afrique est le continent le plus touché : les cas signalés représentent chaque année entre 95 et 99% du total mondial. Le taux global de létalité a été de 2,24%, en 2009, mais a dépassé les 30% parmi les groupes vulnérables résidant dans des zones à haut risque de choléra. Des chiffres bien en dessous de la réalité en raison de la sous-notification des cas, des insuffisances des systèmes de surveillance et de l’absence d’une terminologie normalisée pour la définition d’un cas de choléra. C’est ainsi que, uniquement au Bangladesh, le nombre estimé de cas de choléra survenant chaque année est compris entre 100 000 et 600 000, alors qu’aucun cas n’est notifié à l’OMS. (la fiche de l'institut Pasteur)
Kétamine: Son intérêt en médecine de guerre
Clic sur le document pour accéder au document.
| Tags : kétamine
La trousse de base: Exemple
Elle doit rester SIMPLE, standardisée au sein de l'équipe, permettre l'application du SAFE MARCHE RYAN. Résistez à la tentation d'y introduire du gadget.
Un exemple:
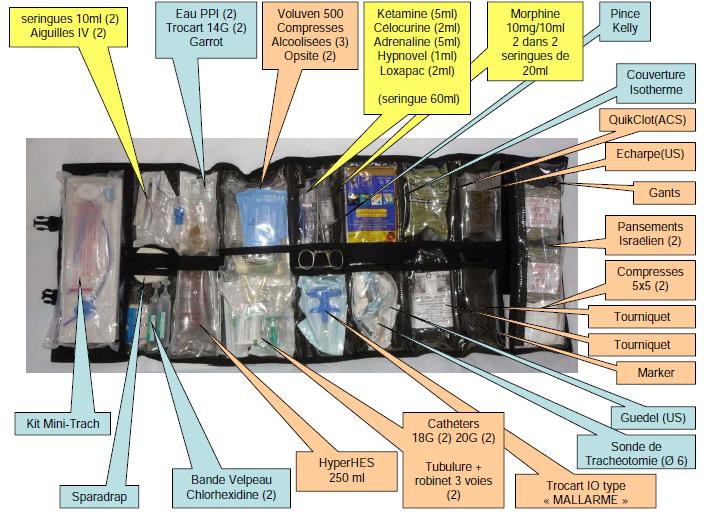
Ne sous estimez pas l'importance de disposer de bandages et d'écharpes en quantité suffisante.
| Tags : trousse
Accélerer une perfusion: Comment ?

Clic sur l'image pour accéder au document
Autotransfusion d'hémothorax; Avec quoi ?
Pas simple en l'absence de matériel dédié. Il s'agit d'une technique qu'il faut avoir anticipé. Une affaire de raccords. Le lien qui suit vous propose une méthode.
10/12/2013
Thoracostomie au doigt: Le mieux !
Simple thoracostomy in prehospital trauma management is safe and effective: a 2-year experience by helicopter emergency medical crews
Massaruttia D et Al. Eur J Emerg Med. 2006 Oct;13(5):276-80
-----------------------------------------------------------------------
La réalisation d'une exsufflation à l'aiguille bien que classique reste discutable du fait de nombreux problèmes techniques et du caractère très relatif de son efficacité. La thoracostomie au doigt doit être considérée comme la technique de référence.
-----------------------------------------------------------------------
OBJECTIVE:
To evaluate the effectiveness and potential complications of simple thoracostomy, as first described by Deakin, as a method for prehospital treatment of traumatic pneumothorax.
METHODS:
Prospective observational study of all severe trauma patients rescued by our Regional Helicopter Emergency Medical Service and treated with on-scene simple thoracostomy, over a period of 25 months, from June 1, 2002 to June 30, 2004.
RESULTS:
Fifty-five consecutive severely injured patients with suspected pneumothorax and an average Revised Trauma Score of 9.6+/-2.7 underwent field simple thoracostomy. Oxygen saturation significantly improved after the procedure (from 86.4+/-10.2% to 98.5%+/-4.7%, P<0.05). No difference exists in the severity of thoracic lesions between patients with systolic arterial pressure and oxygen saturation below and above or equal to 90. A pneumothorax or a haemopneumothorax was found in 91.5% of the cases and a haemothorax in 5.1%. No cases of major bleeding, lung laceration or pleural infection were recorded. No cases of recurrent tension pneumothorax were observed. Forty (72.7%) patients survived to hospital discharge.
CONCLUSIONS:
Prehospital treatment of traumatic pneumothorax by simple thoracostomy without chest tube insertion is a safe and effective technique.
| Tags : pneumothorax
08/12/2013
PTSD et armée anglaise: Touchée comme tout le monde
PTSD in the armed forces: What have we learned from the recent cohort studies of Iraq/Afghanistan?
Goodwin L. et Al. Journal of Mental Health, 2013; 22(5): 397–401
L'armée anglaise semblait préservée du PTSD dans son expérience irakienne: Pas plus de PTSD que dans les troupes non déployées (1). Les explications semblaient se situer au niveau d'une organisation différente (taux d'encadrement, soldats plus âgés, et mission plus courtes). Les choses ont bien changées et actuellement nos alliées sont confrontés aux même problème que nous (2). Il est constaté un taux de PTSD double chez les réservistes engagés (3), par ailleurs ces troubles apparaissent plus tôt et chez des combattants plus jeunes que dans les conflits précédents (4) Le travail présenté fait le point de l'expérience actuelle en la matière des psychiatres militaires anglais
----------------------------------------------
In conclusion, the developments in military epidemiology have allowed cohort studies to confirm that combat experience is temporally related to PTSD. Yet, the majority of those who are deployed seem to be resilient. Across studies there are other common prospective vulnerability factors for PTSD, including psychiatric co-morbidity, alcohol misuse and lack of support. Whilst cross-sectional studies have found evidence to suggest that events outside of the military are important risks for PTSD, this needs to be investigated further in longitudinal research. Delayed-onset PTSD and other symptom trajectories which increase following deployment may be most important from a military perspective, but there is a need to further understand the reasons for the observed heterogeneity of PTSD trajectories.
----------------------------------------------
| Tags : ptsd
Tourniquet abdominal: En théorie cela fonctionne
The Evaluation of an Abdominal Aortic Tourniquet for the Control of Pelvic and Lower Limb Hemorrhage
Taylor D. et Al.Mil Med. 2013;178(11):1196-201
Despite improved body armor, hemorrhage remains the leading cause of preventable death on the battlefield. Trauma to the junctional areas such as pelvis, groin, and axilla can be life threatening and difficult to manage. The Abdominal Aortic Tourniquet (AAT) is a prehospital device capable of preventing pelvic and proximal lower limb hemorrhage by means of external aortic compression. The aim of the study was to evaluate the efficacy of the AAT. Serving soldiers under 25 years old were recruited. Basic demographic data, height, weight, blood pressure, and abdominal girth were recorded. Doppler ultrasound was used to identify blood flow in the common femoral artery (CFA). The AAT was applied while the CFA flow was continuously monitored. The balloon was inflated until flow in the CFA ceased or the maximum pressure of the device was reached. A total of 16 soldiers were recruited. All participants tolerated the device. No complications were reported. Blood flow in the CFA was eliminated in 15 out of 16 participants. The one unsuccessful subject was above average height, weight, body mass index, and abdominal girth. This study shows the AAT to be effective in the control of blood flow in the pelvis and proximal lower limb and potentially lifesaving.
| Tags : hémorragie
07/12/2013
Un modèle de formation hybride ?: A méditer
Evaluation of a training curriculum for prehospital trauma ultrasound.
Press GM et Al. The Journal of Emergency Medicine, Vol. 45, No. 6, pp. 856–864, 2013
BACKGROUND:
In the United States, ultrasound has rarely been incorporated into prehospital care, and scant descriptions of the processes used to train prehospital providers are available.
OBJECTIVES:
Our objective was to evaluate the effectiveness of an extended focused assessment with sonography for trauma (EFAST) training curriculum that incorporated multiple educational modalities. We also aimed to determine if certain demographic factors predicted successful completion.
METHODS:
All aeromedical prehospital providers (APPs) for a Level I trauma center took a 25-question computer-based test to ascertain baseline knowledge. Questions were categorized by content and format. Training over a 2-month period included a didactic course, a hands-on training session, proctored scanning sessions in the Emergency Department, six Internet-based training modules, pocket flashcards, a review session, and remedial training. At the conclusion of the training curriculum, the same test and an objective structured clinical examination were administered to evaluate knowledge gained.
RESULTS:
Thirty-three of 34 APPs completed training. The overall pre-test and post-test means and all content and format subsets showed significant improvement (p < 0.0001 for all). No APP passed the pre-test, and 28 of 33 passed the post-test with a mean score of 78%. No demographic variable predicted passing the post-test. Twenty-seven of 33 APPs passed the objective structured clinical examination, and the only predictive variable was passing the post-test (odds ratio 1.21, 95% confidence interval 1.00-1.25, p = 0.045).
CONCLUSION:
The implementation of a multifaceted EFAST prehospital training program is feasible. Significant improvement in overall and subset testing scores suggests that the test instrument was internally consistent and sufficiently sensitive to capture knowledge gained as a result of the training. Demographic variables were not predictive of test success.
Rupture cricotrachéale: Que faire ?
Cricotracheal Separation after Gunshot to the Neck: Report of a Survivor with Recovery of Bilateral Vocal Fold Function.
Vivero RJ et Al. http://dx.doi.org/10.1016/j.jemermed.2013.08.090
Il s'agit d'une éventualité rarissime mais cette observation montre qu'en situation d'isolement extrême il peut être possible d'agir si la partie distale est visible. Encore faut il connaître l'existence de cette conduite à tenir.
------------------------------------------------------
Initial appropriate airway management is imperative to improve survival. Numerous case reports in the literature demonstrate incidental findings of airway injury after routine workup of the patient or the advent of ominous clinical findings (1,2) . At this stage in patient management, it can become difficult to adequately secure the airway, which places the patient at increased risk. A careful physical examination is therefore critical, with fiberoptic laryngoscopy used, as necessary, in the stable patient. A CT scan can be a useful adjunct in the clinical workup, but it should not be relied upon solely, as it can be inconclusive (3) . When cricotracheal separation is identified and the patient is stable, the airway should be secured surgically in the operating room or trauma bay. The proximal stump of the airway should be grasped and secured with a clamp, and then an awake tracheotomy performed (under local anesthesia if possible) distal to the injury. In the event that the patient is unstable or that intubation fails, the distal stump of the trachea should be identified either visually or by palpation. The stump of trachea should then be grasped with a clamp and pulled superficially (out of the wound toward the skin surface), and an appropriately sized endotracheal tube is placed as a temporary measure and secured. The clamp should not be removed from the airway, as the distal tracheal stump can retract into the mediastinum. The patient should then be taken to the operating room emergently for formal tracheotomy or maturation of the airway tracheostoma. In general, cricothyrotomy should not be performed, as this is usually proximal to the site of airway separation.
| Tags : airway
03/12/2013
Les gelures
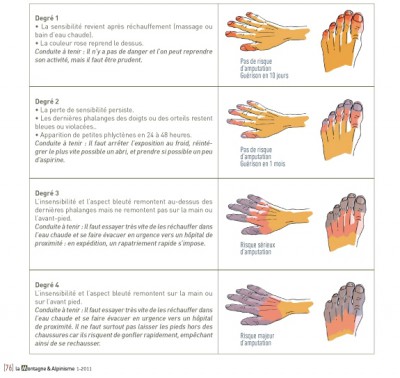
| Tags : gelures
Histoire de température
Clic sur l'image pour accéder au document
| Tags : hypothermie
02/12/2013
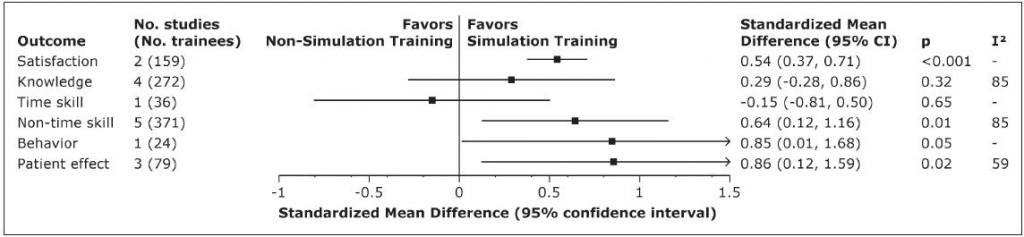
Maîtrise des VAS: Simuler il en restera quelque chose
Advanced Airway Management Simulation Training in Medical Education: A Systematic Review and Meta-Analysis
Kennedy CC et All. Crit Care Med 2013; 41:00–00
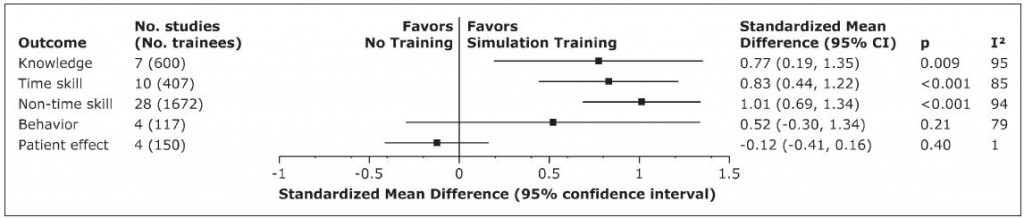
Les quelques lignes qui suivent sont d'une importance cruciale pour la mise en oeuvre d'une politique de formation à la maîtrise des voies aériennes et le maintien de ces compétences. On ne peut être que surpris par l'intérêt modéré de la pratique au bloc opératoire versus la simulation.
------------------------------------------------------------------------
Educators face many choices when designing a curricula—whether to use lecture, video, web-based teaching, and/or simulation. Our findings have substantial implications for educators and researchers. First, educators designing airway education courses can be confident that simulation is effective in comparison with no intervention for most measured outcomes. It also appears to be more effective than non simulation education (e.g., video, lecture, self-study, and OR training) for many educational outcomes. Second, simulation was associated with higher learner satisfaction compared with nonsimulation interventions. Educators designing simulation curricula face further choices, such as which model(s) to use, how to ensure learners retain the skills, and how to provide feedback. This review begins to answer such questions. Learner satisfaction increased with biologic models. Such preferences may be important in designing curriculum, although evidence is presently lacking with regard to the impact on other learning outcomes. Formal training in the OR in addition to simulation training was not associated with benefit. Although evidence is limited, this finding is of considerable practical import given the substantial commitment by OR personnel and potential safety risks incurred by such training. Addition of standardized patients to airway management training likewise does not appear to be beneficial. Finally, curricula that include course repetition, ongoing practice with or without evaluation with feedback, and use of self-regulated learning appear effective in airway management skill retention and should be incorporated for those requiring skills maintenance.
01/12/2013
Cold weather: Epidémio US
Cold weather injuries, active and reserve components, U.S. Armed Forces, July 2008-June 2013.
Armed Forces Health Surveillance Center (AFHSC) MSMR. 2013 Oct;20(10):12-7
Hypothermie Engelures Gelures Pied de tranchée


Facteurs de risque: Jeune, de sexe féminin, ascendance africaine

Rate per 100,000 person-years
| Tags : hypothermie