27/01/2013
Portoir souple: Le SMART XTRACT
Un excellent produit qui permet vraiment de tracter le blessé au sol. Moins d'un kg, bien enveloppant et isolant le blessé de l'environnement. Voir une démo

Noir: 6515-99-297-8494 Vert Olive: 6515-99-297-8494
| Tags : brancardage
Portoir semi-rigide: Pas que le FoxTrot litter et le SKED basic stretcher
Les portoirs semi-rigide ont une place non négligeable pour le transport des blessés. Plus lourds que les portoirs souples, ils ont pour avantage de permettre une meilleure traction au sol et une meilleure protection des blessés? Pour certains ils peuvent même permet,tre un treuillage. Le MEDSLED est un produit particulièrement intéressant.

NSN: 6530-01-608-3195
| Tags : brancardage
26/01/2013
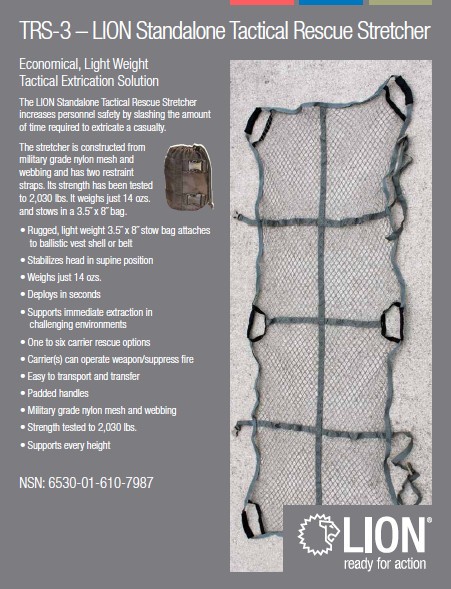
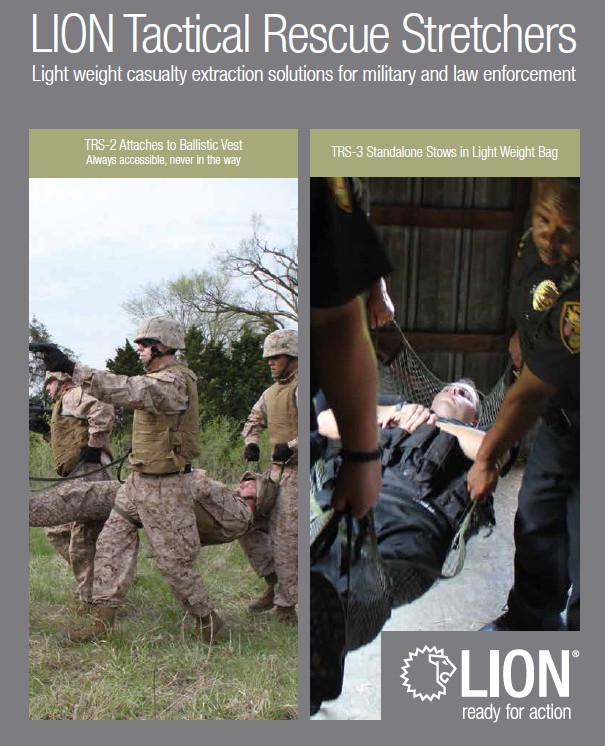
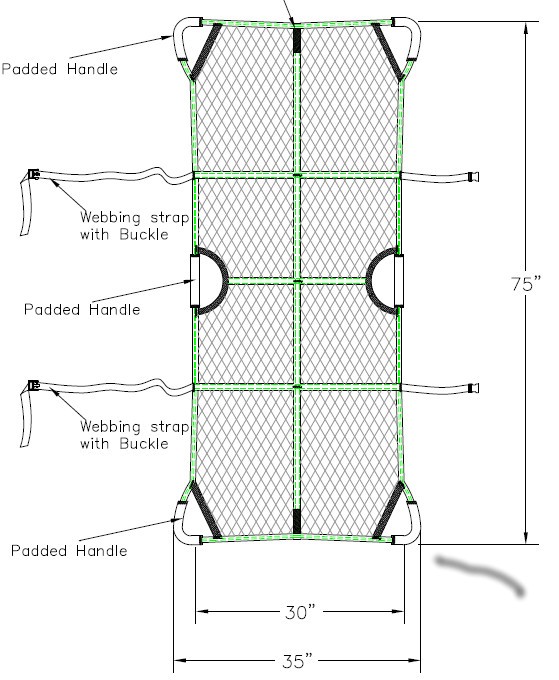
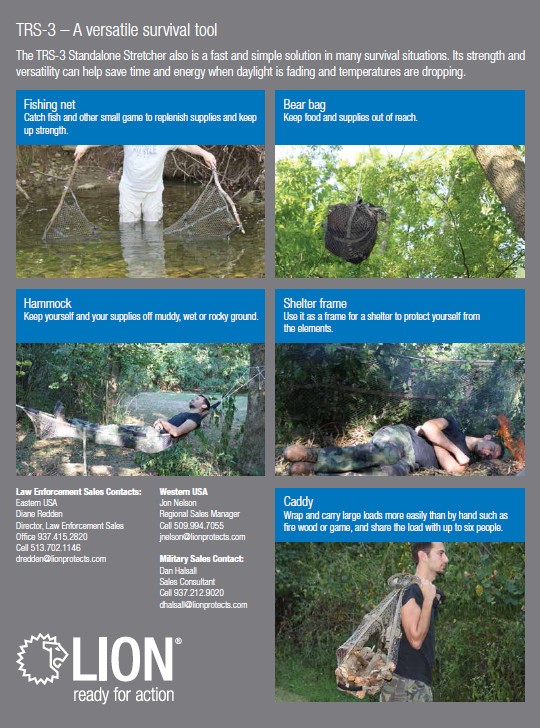
Filet d'extraction: Un nouveau venu
Le filet golanis dimatex est un portoir souple dont la caractéristique principale est son poids très réduit. Il permet une extraction de blessés sur de courtes distances. La limite de ce type de dispositif tient à une préhension difficile sur de longues distances. Un nouveau filet est proposé par EMD Pro. Il apparait être plus polyvalent et propose un système de poignée optilmisé. Portage manuel, harnais, fliet d'extraction, portoir souple type toile à parachute, portoir semi rigide type Fox Trott Litter, portoir rigide type SKEDCO ou, brancard métallique type Talon et barquette aéro type Ferno représentent une gamme de moyens de portage qui doit être disponible en combat moderne.
| Tags : brancardage
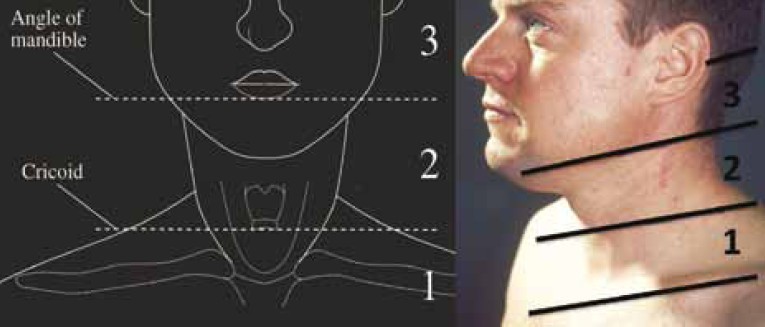
Lésions du cou: Le point UK
Outcomes from Penetrating Ballistic Cervical Injury
Breeze J et all.J R Army Med Corps 158(2): 96-100
Aims:
Ballistic cervical injury has become a significant source of both morbidity and mortality for the deployed UK soldier. The aim of this paper was to document a case series of ballistic cervical wounds to describe the pattern of these injuries and relate them to outcome.
Methods:
The records of all UK service personnel sustaining wounds to the neck in Iraq or Afghanistan between 01 August 2004 and 01 January 2008 were analysed following identification by the Joint Theatre Trauma Registry. Blunt or thermal injuries were excluded.
Results:
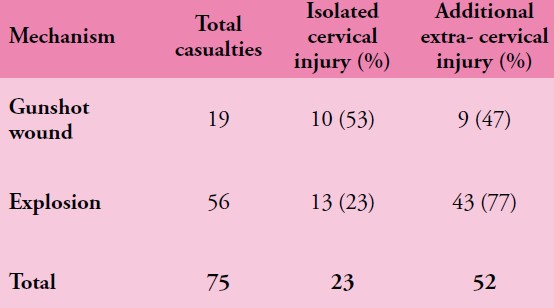
The records of 75/76 service personnel sustaining penetrating cervical injury during this period were available for analysis. 56/75 (75%) were due to explosive fragmentation and the remainder due to gunshot wounds (GSW). 33/75 (44%) of soldiers sustained vascular injury, 32/75 (43%) injury to the spine or spinal cord, 29/75 (39%) injury to the larynx or trachea and 11/75 (15%) injury to the pharynx or oesophagus. 14/75 (19%) patients in this series underwent surgery in a hospital facility for treatment of potentially life threatening cervical injuries, with a survival rate after surgery of 12/14 (86%). The overall mortality from this series of battlefield penetrating neck injury was 63%.

Conclusions:
Penetrating cervical ballistic injury is a significant source of injury to deployed UK service personnel, predominantly due to neurovascular damage. Neck collars if worn would likely prevent many of the injuries in this case series but such protection is uncomfortable and may interfere with common military tasks. Newer methods of protecting the neck should be investigated that will be acceptable to the deployed UK soldier.
| Tags : maxillo, cou, balistique
24/01/2013
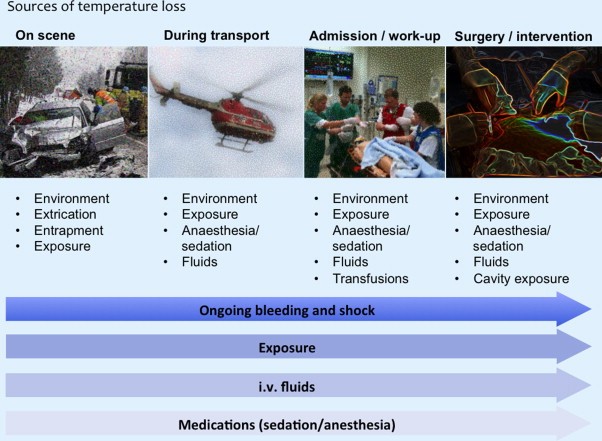
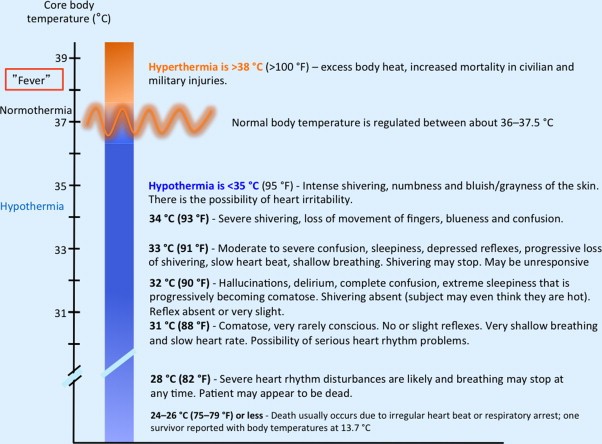
Hypothermie et trauma: Un point 2013
Clinical and translational aspects of hypothermia in major trauma patients: From pathophysiology to prevention, prognosis and potential preservation
http://dx.doi.org/10.1016/j.injury.2012.12.027
_______________________________
Un revue très synthétique à lire, notamment le paragraphe portant sur le recours à une hypothermie induite en cas de traumatisme sévère.
_______________________________
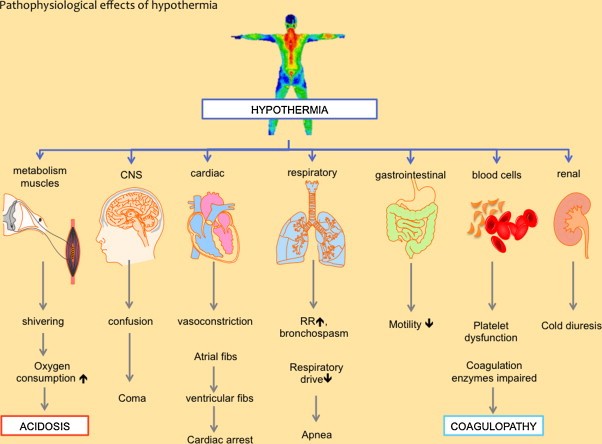
Generally, hypothermia is defined as a core temperature <35°C. In elective surgery, induced hypothermia has beneficial effects. It is recommended to diminish complications attributable to ischemia reperfusion injury. Experimental studies have shown that hypothermia during hemorrhagic shock has beneficial effects on outcome. In contrast, clinical experience with hypothermia in trauma patients has shown accidental hypothermia to be a cause of posttraumatic complications. The different etiology of hypothermia might be one reason for this disparity because induced therapeutic hypothermia, with induction of poikilothermia and shivering prevention, is quite different from accidental hypothermia, which results in physiological stress. Other studies have shown evidence that this contradictory effect is related to the plasma concentration of high-energy phosphates (e.g., adenosine triphosphate [ATP]). Induced hypothermia preserves ATP storage, whereas accidental hypothermia causes depletion. Hypothermia also has an impact on the immunologic response after trauma and elective surgery by decreasing the inflammatory response. This might have a beneficial effect on outcome. Nevertheless, posttraumatic infectious complications may be higher because of an immunosuppressive profile. Further studies are needed to investigate the impact of induced hypothermia on outcome in trauma patients.
_______________________________
Quatre plaques pour une lecture rapide

| Tags : hypothermie
19/01/2013
Hémorragies jonctionnelles: De quoi dispose-t-on en préhospitalier ?
La prise en charge d'hémorragies jonctionnelles est une véritable gageure en préhospitalier. Si ces hémorragies ne sont pas garrotables encore peut-on espérer d'en réduire le débit par la compression directe en ayant recours à l'association de packing de plaies, pansement hémostatiques et pansements compressifs. Depuis peu certains dispositifs mécaniques sont proposés bien que n'ayant pas fait l'objet de validation réelle. Une simple image vaut plus que de long commentaires, alors imprégnez vous de celles-ci.
1. Réaliser un pansement compressif:

Souvenez vous que vous devez disposer de pansement et que vous devez être en capacités de réaliser un pansement de ce type sur une racine de membres. Il doit être associer rembourage de toute cavité avec ce que vous avez sous la main, idéalement pansement hémostatique au contact de ce qui saigne et COMPRESSION forte.
2. Comprimer l'aorte abdominale:
Le garrot abdominal (The Abdominal Aortic Tourniquet)

Ce dispositif existe depuis plusieurs années. Il a une assisse expérimentale mais n'est pas diffusé. On pourrait l'assimiler grossièrement au compartiment abdominal du pantalon antichoc
3. Comprimer l'artère fémorale au pli inguinal
Le CROC: (Combat Ready Clamp)

Ce dispsositif a été validé par l'armée US qui vient de l'intégrer au TCCC.
Le JETT (Junctional Emergency Treatment Tool)

Ce dispositif vient d'être présenté et semble être efficace
Lire aussi ce document
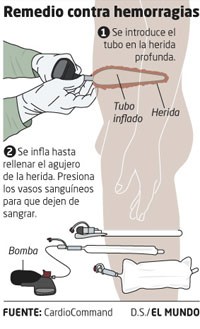
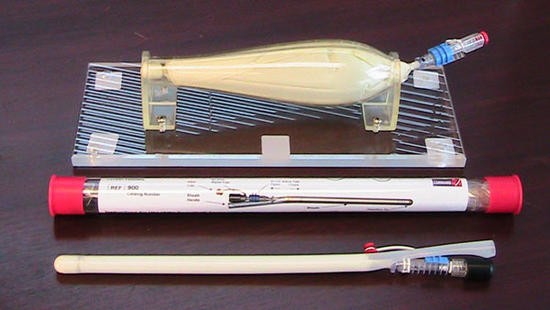
4. Réaliser l'équivalent d'un packing de plaie
Le principe est d'insérer un ballon que l'on gonfle dans la cavité. Ceci est faisable avec une sonde de foley, mais dans ce cas le ballon est de bien plus grand volume.
5. Comprimer directement la zone hémorragique par un clamp

02/01/2013
Kétamine: La bonne dose pour le bon usage
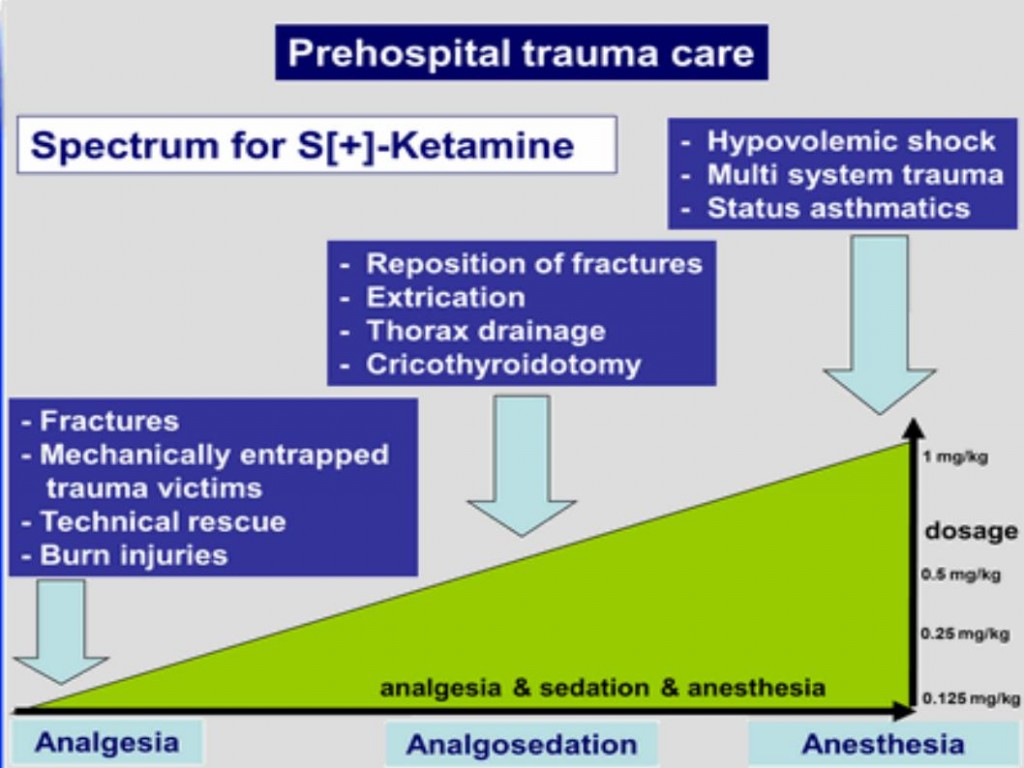
Josse F SOMA 2011
01/01/2013
SOTECH
![]()