Emergency physicians were trained in the use of Ezt on manikins. Ten consecutive successful intubations were required for every physician before beginning the evaluation of Ezt.
The inclusion criteria were: all the patients with a height above 90 cm and an indication for prehospital airway management.
The exclusion criteria were a contraindication to the use of Ezt: patients with a height less than 90 cm, patients suffering from upper airway obstruction, and patients suffering from oesophageal diseases or ingestion of caustic substances.
2.3. Protocol
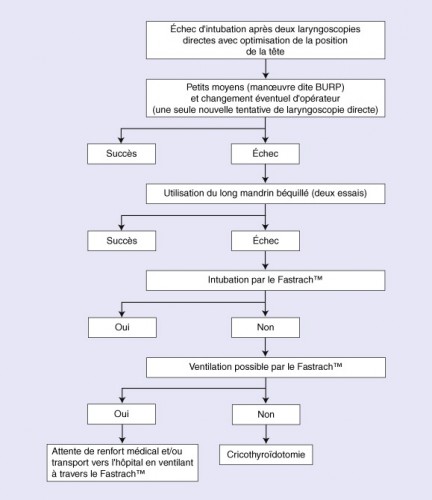
During the study period, all patients were managed with the same airway management protocol (Fig. 2). Our protocol complies with the guidelines of the French Society of Anaesthesia and Resuscitation (SFAR) and received ethical approval from Marseille University Hospital's Emergency Committee.
The SFAR defines difficult intubation (DI) as more than two failed intubation attempts under direct laryngoscopy with an optimal head position.
We prospectively separated patients into 2 groups: “easy airway management”: less than 2 ETI attempts and “difficult airway management”: more than 2 ETI attempts or use of EZT in accordance with the protocol.
In our study, before ETI we also systematically evaluate predictive signs of DI (short neck, restricted mouthopening <3 cm, estimated thyromental distance <6 cm, morbid obesity with body mass index estimated more than 40 and cervico-facial trauma).
For a patient with vital distress on arrival of the prehospital medical team on-site and after evaluation of the situation, the emergency physician decides if intubation is necessary.
The patients were preoxygenated by Bag–Valve–Mask (BVM) with 100% oxygen for 3 min, except in the case of cardio-respiratory arrest or if there was an immediate indication of intubation.
During airway management, patients were monitored continuously by electrocardiogram, cutaneous pulse oximetry and non-invasive arterial pressure.
A Rapid Sequence Induction (RSI) with etomidate (0.3 mg/kg) and succinylcholine (1 mg/kg) was performed in patients with cardiac activity. Arrest patients were intubated without giving any medications.
If there was no predictive sign of DI, ETI was attempted with an ETT and by a direct laryngoscopy, with or without a stylet.
Whatever the attempted airway management, this is always limited to 40 s.
If ETI failed, ventilation by BVM with 100% oxygen was resumed, or in the event of a predictive sign of DI, an attempt at ETI was recommended but with measures taken to facilitate intubation: place the head in the modified Jackson position or “sniffing position”, if no cervico-facial trauma, bend the tube into a “hockey stick” shape with a stylet and have an assistant perform the BURP (backward upward rightward pressure) maneuver to move the larynx closer to the visual axis for intubation.
If ETI failed again, ventilation by BVM with 100% oxygen was resumed and a further attempt with Ezt was recommended, respecting any contraindications.
If a “cannot intubate, cannot ventilate” situation occurred and as no time could be wasted in further intubation attempts, immediate use of Ezt was allowed because the Combitube and the Ezt are listed as a rescue method in “cannot ventilate–cannot intubate” situations by the American Society of Anaesthesiologists [6].
Laryngoscopic insertion of Ezt is very similar to the use of a standard ETT, and if an ETI by Ezt is finally possible, the patient is ventilated through the transparent lumen.
If ETI is not possible, the tip of the EzT can be inserted into the esophagus under visual guidance with the help of a laryngoscope or blindly.
If it is inserted blindly, the patient's head must be in neutral position. Manually opening the patient's mouthand pressing the tongue gently toward the mandible, the tube is inserted parallel to the frontal axis of the patient until the proximal black ring mark is positioned at the level of the incisors. If the EzT is inserted blindly, the tip is likely to be positioned in the esophagus with a probability of more than 95% [3]. Ventilation of the patient should be performed using a colored lumen, and the transparent lumen can then be used to insert a gastric tube or to drain gastric contents.
The colored pharyngeal proximal cuff and the transparent distal cuff are subsequently inflated with 80 and 10 ml of air, using two pre-filled syringes in the package. Inflation of the pharyngeal cuff occludes theoropharynx and should prevent inhalation of blood or secretions from the oral or nasal cavity. The transparentdistal cuff seals the oesophagus and should prevent inhalation of gastric contents.
Correct insertion of Ezt was defined as efficient ventilation of the patient assessed by three square-wave capnograph traces during manual ventilation, symmetric auscultation with no audible gastric insufflations or air leak.
If all of these methods failed, ventilation by BVM with 100% oxygen was resumed and a “Failed Airway Algorithm” was applied to the patients by performing a cricothyrotomy with the “Quick-Trach Emergency Cricothyrotomy Device.”
After airway management, anaesthesia was maintained with Midazolam (0.1 mg/kg/h) and Fentanyl(1 μg/kg/h). The patients underwent positive pressure ventilation in a pressure-controlled mode; the limit was set at 30 cm H2O airway pressure; the targeted tidal volume was 7 mL/kg; inspired oxygen concentration (FIO2) at 1; respiratory rate was set to achieve an End-Tidal CO2 (ETCO2) concentration of 35–45 mmHg. The patients were continuously monitored by standard non-invasive measures including electrocardiogram, cutaneous pulse oximetry, non-invasive blood pressure measurement (every 5 min) and capnography.
Subsequently, the patients were rapidly admitted to intensive care unit (ICU). The Ezt was replaced by an ETT in ICU, with an airway exchange catheter as soon as possible.
2.4. Data collection and measurements
The emergency physicians filled the study forms immediately after each airway management. The study form included patient's age and sex, Glasgow coma scale (GCS) score, approximate height (less or more than 130 cm), clinical status and indication for intubation (cardio-respiratory arrest, severe neurological distress, severe respiratory distress or other). The forms were anonymous. Predictive signs of DI (short neck, restricted mouth opening <3 cm, estimated thyromental distance <6 cm, morbid obesity and cervico-facialtrauma) and number of intubation attempts were also noted. Incidents and complications of intubation were reported by means of open-ended questions. All the data were then managed in a computer database.
3. Results
During the study period, 239 patients needed prehospital airway management and no patient was excluded.
These 239 patients were divided into 2 groups: 225 (94%) patients in “easy airway management” and 14 (6%) patients in “difficult airway management”. The characteristics for both groups are illustrated in Table 1.