17/12/2010
Quel laryngoscope ?
Le choix d'un laryngoscope "tactique" n'est pas simple. C'est un compromis entre la modalité choisie de contrôle des voies aériennes (pas d'intubation, coniotomie ou intubation ?), le poids du laryngoscope, la taille de la lame et les qualités optiques attendues.
Vous dispsoez outre de la boite d'intubation standard du laryngoscope trulite de la société truphatek.

Il a été choisi d'approvionner ce laryngoscope en lame fixe de taille 3 qui semble la plus polyvalente. Ce laryngoscope est remarquable de part sa légèreté, la présence d'un manche court et la qualité de la lumière LED fournie. Il est en principe à patient unique.
Pour pallier au problème du choix de la taille de la lame, certains proposent des produits originaux. Ainsi le duoscope de la société PARKER propose deux tailles de lame et un éclairage de grande qualité. sa manipulation est moins aisée car c'est la seconde lame qui sert de manche.
| Tags : intubation, airway
14/12/2010
Abord des voies aériennes:Que font les anglais ?
10 % des blessés évacués nécessite une intubation dont 4.7% avant l'embarquement dans le vecteur d'évacuation. Dans ce travail la limite est que nous ne savons pas ce qui relève de blessés au combat , s'il s'agit de blessés militaires, de la répartition des procédures en fonction du contexte. Dans de telles conditions la prise en charge de patients/blessés en arrêt circulatoire est vaine .
J R Army Med Corps. 2010 Sep;156(3):159-61.
Advanced airway management--a medical emergency response team perspective.
Selly Oak Hospital, Birmingham. aghaldane1@doctors.org.uk
Abstract
OBJECTIVES: To determine the number of medical emergency response team (MERT) patients undergoing advanced airway management in the peri-evacuation phase and to determine the indications for airway interventions undertaken in flight.
METHODS: This was a retrospective study. Data was collected from patient report and mission debrief forms completed after each MERT mission during Operation HERRICK 10 (April-October 2009). All patients that received advanced airway interventions before or during evacuation were identified.
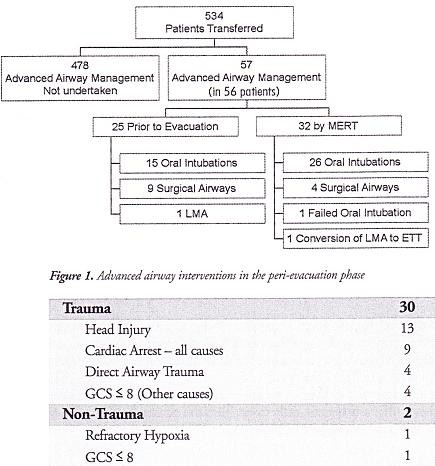
RESULTS: MERTs were involved in the primary transfer of 534 patients during the period studied, 56 (10.5%) underwent advanced airway management, of which 31 (5.8% of total) were initiated by the MERT in the peri-evacuation phase. Twenty five cases (4.7%) underwent advanced airway management by other pre-hospital providers prior to MERT arrival. Of the 31 advanced airway interventions undertaken in-flight, cardiac arrest was the primary indication in only nine cases.
CONCLUSIONS: The figure of 56 patients requiring advanced airway management is at the higher end of the range expected from the study of historical military data. This may reflect the doctrine of "intelligent tasking", that is sending this physician-led team to the most seriously injured casualties.
Morceaux choisis
1. Intubation et coniotomie sont la base
2. Les indications diffèrent de la médecine préhospitalière civile
"..
The indications for those advanced airway interventions undertaken by the MERT is in keeping with the historical data: Head injury making the biggest group once those inrubated for post-operative resplratory support ie those transferred post-operatively from an FST location rather than direct from the point of wounding are excluded . The majoriry of the cases were trauma (93,5%) with the remaining non-traula causes (6,5%) (table 1); This figure is again similar io the recent US study [11].
.."
| Tags : airway, intubation