06/02/2026
Foley ou Seringue ?
16/02/2023
Guerre Hybride: Position du problème
Hybrid warfare and counter-terrorism medicine
Derrick Tin D et Al.. Eur J Trauma Emerg Surg. 2023 Feb 10;1-5.
Introduction:
March 9, 2022. An airstrike by Russian forces destroying a maternity hospital in Mariupol, Ukraine. The image of a severely injured pregnant woman covered in blood being stretchered away against the backdrop of destroyed buildings. Mutterings of the use of chemical weapons. This paper is a primer for healthcare personnel and health systems on hybrid warfare and counter-terrorism medicine.
Discussion:
While recent events and images arising from conflicts around the world represent a cruel hallmark in today's history, attacks against healthcare facilities and innocent civilians are not new and continue to be perpetrated around the world. In war, the Geneva Convention protects civilians and healthcare institutions from harm but when war crimes are being committed and civilians knowingly targeted, parallels from a healthcare perspective can be drawn with terrorism events. Increasingly, civilian institutions and in particular the healthcare sector, are drawn into such conflicts and understanding the health system impact of hybrid warfare and other asymmetrical attack methods is of great importance.
Conclusion:
The field of Counter-Terrorism Medicine (CTM) explores the healthcare impacts of intentional, man-made attacks and much recent research and discussions around this topic are extremely relevant and applicable not just to the ongoing hybrid war in Ukraine, but to today's threat climate all around us.
12/11/2022
Histoire d'effets de protection
Warfighter Personal Protective Equipment and Combat Wounds
Background:
Personal protective equipment (PPE) is crucial to force protection and preservation. Innovation in PPE has shifted injury patterns, with protected body regions accounting for decreased proportions of battlefield trauma relative to unprotected regions. Little is known regarding the PPE in use by warfighters at the time of injury.
Methods:
We queried the Prehospital Trauma Registry (PHTR) for all encounters from 2003-2019. This is a sub-analysis of casualties with documented PPE at the time of medical encounter. When possible, encounters were linked to the Department of Defense Trauma Registry (DODTR) for outcome data. Serious injuries are defined as an abbreviated injury scale of 3 or greater.
Results:
Of 1,357 total casualty encounters in the PHTR, 83 were US military with documented PPE. We link 62 of this cohort to DODTR. The median composite Injury Severity Score (ISS) was 6 (Interquartile range (IQR) 4-21), and 11 casualties (18%) had an ISS >25. The most seriously injured body regions were the extremities (21%), head/neck (16%), thorax (16%), and abdomen (10%). PPE worn at time of injury included helmet (91%), eye protection (73%), front (75%) and rear plates (77%), left/right plates (65%), tactical vest (46%), groin protection (12%), neck protection (6%), pelvic shield (3%), and deltoid protection (3%).
Conclusion:
Our data set demonstrates that the extremities were the most commonly injured body region, followed by head/neck, and thorax. PPE designed for the extremities and neck are also among the least commonly worn protective equipment.
07/04/2022
Connaître les UXO
![]()
Clic sur l'image
12/04/2021
KIA pour les UK en Afghanistan
Killed in action (KIA): an analysis of military personnel who died of their injuries before reaching a definitive medical treatment facility in Afghanistan (2004-2014)
Introduction: The majority of combat deaths occur before arrival at a medical treatment facility but no previous studies have comprehensively examined this phase of care.
Methods: The UK Joint Theatre Trauma Registry was used to identify all UK military personnel who died in Afghanistan (2004-2014). These data were linked to non-medical tactical and operational records to provide an accurate timeline of events. Cause of death was determined from records taken at postmortem review. The primary objective was to report time between injury and death in those killed in action (KIA); secondary objectives included: reporting mortality at key North Atlantic Treaty Organisation timelines (0, 10, 60, 120 min), comparison of temporal lethality for different anatomical injuries and analysing trends in the case fatality rate (CFR).
Results: 2413 UK personnel were injured in Afghanistan from 2004 to 2014; 448 died, with a CFR of 18.6%. 390 (87.1%) of these died prehospital (n=348 KIA, n=42 killed non-enemy action). Complete data were available for n=303 (87.1%) KIA: median Injury Severity Score 75.0 (IQR 55.5-75.0). The predominant mechanisms were improvised explosive device (n=166, 54.8%) and gunshot wound (n=96, 31.7%).In the KIA cohort, the median time to death was 0.0 (IQR 0.0-21.8) min; 173 (57.1%) died immediately (0 min). At 10, 60 and 120 min post injury, 205 (67.7%), 277 (91.4%) and 300 (99.0%) casualties were dead, respectively.

Whole body primary injury had the fastest mortality. Overall prehospital CFR improved throughout the period while in-hospital CFR remained constant.
Conclusion: Over two-thirds of KIA deaths occurred within 10 min of injury. Improvement in the CFR in Afghanistan was predominantly in the prehospital phase.
09/02/2020
Tuerie de masse ou violence urbaine: Vite vers l'hôpital !
Comparison of the causes of death and wounding patterns in urban firearm-related violence and civilian public mass shooting events.
BACKGROUND:
There are no reports comparing wounding pattern in urban and public mass shooting events (CPMS). Because CPMS receive greater media coverage, there is a connation that the nature of wounding is more grave than daily urban gun violence. We hypothesize that the mechanism of death following urban gunshot wounds (GSWs) is the same as has been reported following CPMS.
METHODS:
Autopsy reports of all firearm-related deaths in Washington, DC were reviewed from January 1, 2016, to December 31, 2017. Demographic data, firearm type, number and anatomic location of GSWs, and organ(s) injured were abstracted. The organ injury resulting in death was noted. The results were compared with a previously published study of 19 CPMS events involving 213 victims.
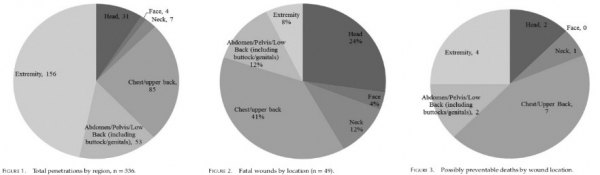
RESULTS:
One hundred eighty-six urban autopsy reports were reviewed. There were 171 (92%) homicides and 13 (7%) suicides. Handguns were implicated in 180 (97%) events. One hundred eight (59%) gunshots were to the chest/upper back, 85 (46%) to the head, 77 (42%) to an extremity, and 71 (38%) to the abdomen/lower back. The leading mechanisms of death in both urban firearm violence and CPMS were injury to the brain, lung parenchyma, and heart. Fatal brain injury was more common in CPMS events as compared with urban events involving a handgun.
CONCLUSION:
There is little difference in wounding pattern between urban and CPMS firearm events. Based on the organs injured, rapid point of wounding care and transport to a trauma center remain the best options for mitigating death following all GSW events.
08/02/2020
Rachis et extraction de véhicules
An explorative, biomechanical analysis of spine motion during out-of-hospital extrication procedures.
Häske D et Al. Injury. 2020 Feb;51(2):185-192.
------------------------------------
Un travail qui interpelle par ses implications potentielles sur la manière d'extraire les combattants de véhicules qu'ils soient terrestres ou aéronautiques.
------------------------------------
OBJECTIVES:
The extrication of patients following a road traffic collision is among the basic procedures in emergency medicine. Thus, extrication is a frequently performed procedure by most of the emergency medical services worldwide. The appropriate extrication procedure depends on the patient's current condition and accompanying injuries. A rapid extrication should be performed within a few minutes, and the cervical spine (at least) should be immobilized. To our knowledge, the scientific literature and current guidelines do not offer detailed recommendations on the extrication of injured patients. Thus, the aim of the current study is to compare the effectiveness of spinal stabilization during various out-of-hospital extrication procedures.
METHODS: This is an explorative, biomechanical analysis of spine motion during different extrication procedures on an example patient. Movement of the cervical spine was measured using a wireless human motion tracker. Movement of the thoracic and lumbar spine was quantified with 12 strain gauge sensors, which were positioned paravertebrally on both sites along the thoracic and lumbar spine. To interpret angular movement, a motionscore was developed based on newly defined axioms on the biomechanics of the injured spine.
RESULTS: Self-extrication showed the least spinal movement (overall motionscore sum = 667). Movement in the cervical spine could further be reduced by applying a cervical collar. The extrication by a rescue boa showed comparable results in overall spinal movement compared to the traditional extrication via spineboard (overall motionscore sum = 1862vs. 1743). Especially in the cervical spine, the spinal movement was reduced (motionscore sum = 339 vs. 595). However, the thoracic spine movement was increased (motionscore sum = 812 vs. 432).
| Self- extrication without a cervical collar | Self- extrication with a cervical collar | Rapid extrication | Rapid extrication with rescue boa | Rapid extrication with a slide board and rescue boa | Rapid extrication with a patient transfer sheet | ||
|---|---|---|---|---|---|---|---|
| C1 – C7 | flexion/extension | 25 | 6 | 117 | 132 | 199 | 27 |
| rotation | 28 | 6 | 287 | 165 | 216 | 32 | |
| lateral bending | 76 | 19 | 191 | 42 | 65 | 52 | |
| sum | 129 | 31 | 595 | 339 | 480 | 111 | |
| Th1 – Th9 | flexion/extension | 18 | 17 | 69 | 91 | 76 | 24 |
| rotation | 157 | 122 | 286 | 598 | 559 | 156 | |
| lateral bending | 65 | 52 | 77 | 123 | 107 | 85 | |
| sum | 240 | 191 | 432 | 812 | 742 | 265 | |
| Th10 – L2 | flexion/extension | 21 | 46 | 83 | 109 | 82 | 43 |
| rotation | 99 | 185 | 146 | 180 | 114 | 114 | |
| sum | 120 | 231 | 229 | 289 | 196 | 157 | |
| L3 – L5 | flexion/extension | 38 | 251 | 143 | 254 | 117 | 25 |
| rotation | 73 | 93 | 286 | 93 | 178 | 64 | |
| lateral bending | 67 | 67 | 58 | 75 | 117 | 102 | |
| sum | 178 | 411 | 487 | 422 | 412 | 191 | |
| Total sum | 667 | 864 | 1743 | 1862 | 1830 | 724 | |
CONCLUSION: In case of a suspected cervical spine injury, guided self-extrication seems to be the best option. If the patient is not able to perform self-extrication, using a rescue boa might reduce cervical spinal movement compared to the traditional extrication procedure. Since promising results are shown in the case of extrication using a patient transfer sheet that has already been placed below the driver, future developments should focus on novel vehicle seats that already include an extrication device.
23/09/2019
+ il y a de couches + c'est important
The effect of military clothing on gunshot wound patterns in a cadaveric animal limb model.
The majority of injuries in survivors of gunshot wounds (GSW) are typically to the extremities. Novel wound ballistic research is encouraged to try and capture corporate knowledge on the management of these injuries gained during recent conflicts and understand the wounding patterns seen. With recent work examining the effect of UK military clothing on extremity GSW patterns in a synthetic model, a model with greater biofidelity is needed for ballistic testing. The aim of this study was to assess the effect of UK military clothing on GSW patterns within a cadaveric animal limb model using two types of ammunition commonly used in recent conflicts-7.62 × 39 mm and 5.45 × 39 mm. In total, 24 fallow deer hind limbs were shot, 12 by 7.62 mm projectiles and the remaining 12 shot by 5.45 mm projectiles, further divided into four with no clothing layers (Cnil), four with a single clothing layer (Cmin) and four with maximum clothing layers (Cmax) as worn on active duty by UK military personnel. Limbs were analysed after ballistic impact using contrast CT scanning to obtain measurements of permanent cavity damage, and results were compared using analysis of variance (ANOVA).
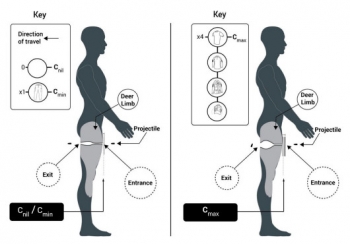
Results showed significantly different damage measurements within limbs with Cmax for both ammunition types compared with the other clothing states. This may result in GSWs that require more extensive surgical management, and invites further study.
17/09/2019
Violences urbaines et tueries massives: Des profils proches ?
Comparison of the Causes of Death and Wounding Patterns in Urban Firearm-Related Violence and Civilian Public Mass Shooting Events.
BACKGROUND:
There are no reports comparing wounding pattern in urban and public mass shooting events (CPMS). Because CPMS receive greater media coverage, there is a connation that the nature of wounding is more grave than daily urban gun violence. We hypothesize that the mechanism of death following urban GSWs is the same as has been reported following CPMS.
METHODS:
Autopsy reports of all firearm related deaths in Washington, DC were reviewed from January 1, 2016 to December 31, 2017. Demographic data, firearm type, number and anatomic location of GSWs, and organ(s) injured were abstracted. The organ injury resulting in death was noted. The results were compared to a previously published study of 19 CPMS events involving 213 victims.
RESULTS:
186 urban autopsy reports were reviewed. There were 171 (92%) homicides and 13 (7%) suicides. Handguns were implicated in 180 (97%) events. One hundred eight gunshots (59%) were to the chest/upper back, 85 (46%) to the head, 77 (42%) to an extremity, and 71 (38%) to the abdomen/lower back. The leading mechanisms of death in both urban firearm violence and CPMS were injury to the brain, lung parenchyma, and heart. Fatal brain injury was more common in CPMS events as compared to urban events involving a handgun.
CONCLUSION:
There is little difference in wounding pattern between urban and CPMS firearm events. Based on the organs injured, rapid point of wounding care and transport to a trauma center remain the best options for mitigating death following all GSW events.
15/09/2019
Tueries par armes à feu: Causes évitables de décès
Fatal Wounding Pattern and Causes of Potentially Preventable Death Following the Pulse Night Club Shooting Event.
Smith ER et Al. Prehosp Emerg Care. 2018 Nov-Dec;22(6):662-668.
---------------------------------------
Cet article confirme que la nécessité d'une organisation spécifique de la prise en charge des victimles de terrorisme. La répartition des causes évitables de décès après tirs d'armes à feu diffère quelque peu des problématiques militaires. La probabilité de survie est moindre. Si la stratégie de pose précoce du garrot est importante, elle n'est pas suffisante. Ainsi il est rapporté qu'un tiers des décès pourrait être évités, que si des exsanguinations liées à des atteintes des membres sont observées, les causes thoraciques apparaissent être une cible de prise en charge précoce notamment par exsufflation de pneumothorax compressif dont l'occurence apparaît plus fréquente qu'en milieu militaire.
---------------------------------------
BACKGROUND:
Mortality following shooting is related to time to provision of initial and definitive care. An understanding of the wounding pattern, opportunities for rescue, and incidence of possibly preventable death is needed to achieve the goal of zero preventable deaths following trauma.
METHODS:
A retrospective study of autopsy reports for all victims involved in the Pulse Nightclub Shooting was performed. The site of injury, probable site of fatal injury, and presence of potentially survivable injury (defined as survival if prehospital care is provided within 10 minutes and trauma center care within 60 minutes of injury) was determined independently by each author. Wounds were considered fatal if they involved penetration of the heart, injury to any non-extremity major blood vessel, or bihemispheric, mid-brain, or brainstem injury.
RESULTS:
There were an average of 6.9 wounds per patient. Ninety percent had a gunshot to an extremity, 78% to the chest, 47% to the abdomen/pelvis, and 39% to the head. Sixteen patients (32%) had potentially survivable wounds, 9 (56%) of whom had torso injuries. Four patients had extremity injuries, 2 involved femoral vessels and 2 involved the axilla. No patients had documented tourniquets or wound packing prior to arrival to the hospital.
One patient had an isolated C6 injury and 2 victims had unihemispheric gunshots to the head.
CONCLUSIONS:
A comprehensive strategy starting with civilian providers to provide care at the point of wounding along with a coordinated public safety approach to rapidly evacuate the wounded may increase survival in future events.
24/07/2019
Examiner un bassin: Peu faible en préhospitalier
Clinical Examination of the Pelvic Ring in the Prehospital Phase.
INTRODUCTION:
Instable pelvic fractures are associated with significant hemorrhage and shock. Instability of the pelvic ring should be tested with the manual compression test (MCT) and instable pelvic ring fractures should prompt mechanical stabilization. However, the accuracy of the prehospital MCT in patients, that sustained a high energetic trauma, is still unknown.
SETTING:
Radboudumc Nijmegen, level 1 trauma center, the Netherlands.
METHODS:
This prospective blind observational study included all patients after a high impact blunt trauma treated by an experienced Helicopter Emergency Medical Service (HEMS) physician. Nominal arranged questionnaires were filled in by the HEMS physician prior to the radiological examination of the patient.
RESULTS:
We included 56 patients of which 11 sustained a pelvic ring fracture. 13 patients were treated with pelvic compression devices, of which only five patients had a pelvic ring fracture. Prehospital performed clinical examination by the HEMS physicians had an overall sensitivity of 0.45 (95% CI 0.16-0.75) and a specificity of 0.93 (95% CI 0.29-0.96).
CONCLUSION:
Pelvic ring instability cannot accurately be diagnosed in the prehospital setting, based on the MCT. The use of the pelvic binder should standard in high impact blunt trauma patients, independently of the MCT or trauma mechanism.
| Tags : pelvis
12/12/2018
Tueries massives: Une distribution différente des blessures de guerre
Fatal Wounding Pattern and Causes of Potentially Preventable Death Following the Pulse Night Club Shooting Event.
--------------------------------
BACKGROUND:
Mortality following shooting is related to time to provision of initial and definitive care. An understanding of the wounding pattern, opportunities for rescue, and incidence of possibly preventable death is needed to achieve the goal of zero preventable deaths following trauma.
METHODS:
A retrospective study of autopsy reports for all victims involved in the Pulse Nightclub Shooting was performed. The site of injury, probable site of fatal injury, and presence of potentially survivable injury (defined as survival if prehospital care is provided within 10 minutes and trauma center care within 60 minutes of injury) was determined independently by each author. Wounds were considered fatal if they involved penetration of the heart, injury to any non-extremity major blood vessel, or bihemispheric, mid-brain, or brainstem injury.
RESULTS:
There were an average of 6.9 wounds per patient. Ninety percent had a gunshot to an extremity, 78% to the chest, 47% to the abdomen/pelvis, and 39% to the head. Sixteen patients (32%) had potentially survivable wounds, 9 (56%) of whom had torso injuries. Four patients had extremity injuries, 2 involved femoral vessels and 2 involved the axilla. No patients had documented tourniquets or wound packing prior to arrival to the hospital. One patient had an isolated C6 injury and 2 victims had unihemispheric gunshots to the head.
CONCLUSIONS:
A comprehensive strategy starting with civilian providers to provide care at the point of wounding along with a coordinated public safety approach to rapidly evacuate the wounded may increase survival in future events.
Tueries massives: Une distribution différente des blessures de guerre
Fatal Wounding Pattern and Causes of Potentially Preventable Death Following the Pulse Night Club Shooting Event.
--------------------------------
BACKGROUND:
Mortality following shooting is related to time to provision of initial and definitive care. An understanding of the wounding pattern, opportunities for rescue, and incidence of possibly preventable death is needed to achieve the goal of zero preventable deaths following trauma.
METHODS:
A retrospective study of autopsy reports for all victims involved in the Pulse Nightclub Shooting was performed. The site of injury, probable site of fatal injury, and presence of potentially survivable injury (defined as survival if prehospital care is provided within 10 minutes and trauma center care within 60 minutes of injury) was determined independently by each author. Wounds were considered fatal if they involved penetration of the heart, injury to any non-extremity major blood vessel, or bihemispheric, mid-brain, or brainstem injury.
RESULTS:
There were an average of 6.9 wounds per patient. Ninety percent had a gunshot to an extremity, 78% to the chest, 47% to the abdomen/pelvis, and 39% to the head. Sixteen patients (32%) had potentially survivable wounds, 9 (56%) of whom had torso injuries. Four patients had extremity injuries, 2 involved femoral vessels and 2 involved the axilla. No patients had documented tourniquets or wound packing prior to arrival to the hospital. One patient had an isolated C6 injury and 2 victims had unihemispheric gunshots to the head.
CONCLUSIONS:
A comprehensive strategy starting with civilian providers to provide care at the point of wounding along with a coordinated public safety approach to rapidly evacuate the wounded may increase survival in future events.
21/07/2018
AP-IED: +grave que mine
Injury profile suffered by targets of antipersonnel improvised explosive devices: prospective cohort study
Victims of AP-IED were more likely, compared with APM victims, to have multiple amputations (70.0% vs 10.4%; p<0.001) or genital injury (26% vs 13%; p=0.007). Multiple amputations occurred in 70 patients: 5 quadruple amputations, 27 triple amputations and 38 double amputations. Pelvic fracture occurred in 21 victims, all but one of whom had multiple amputations. Severe perineal, gluteal or genital injuries were present in 46 patients. Severe soft tissue injury was universal, with injection of contaminated soil along tissue planes well above entry sites. There were 13 facial injuries, 9 skull fractures and 3 traumatic brain injuries. Eleven eye injuries were seen; none of the victims with eye injuries were wearing eye protection. The casualty fatality rate was at least 19%. The presence of more than one amputation was associated with a higher rate of pelvic fracture (28.6% vs 3.3%; p=0.005) and perineal–gluteal injury (32.6% vs 11.1%; p=0.009).
The injury pattern suffered by the target of the AP-IED is markedly worse than that of conventional APM. Pelvic binders and tourniquets should be applied at the point of injury to patients with multiple amputations or perineal injuries.
| Tags : blast
06/02/2018
Gilet de protection: A porter près du corps
Do air-gaps behind soft body armour affect protection?
INTRODUCTION:
Body armour typically comprises a fabric garment covering the torso combined with hard armour (ceramic/composite). Some users wear only soft armour which provides protection from sharp weapons and pistol ammunition. It is usually recommended that body armour is worn against the body with no air-gaps being present between the wearer and the armour. However, air-gaps can occur in certain situations such as females around the breasts, in badly fitting armour and where manufacturers have incorporated an air-gap claiming improvements in thermophysiological burden. The effect of an air-gap on the ballistic protection and the back face signature (BFS) as a result of a non-perforating ballistic impact was determined.
METHODS:
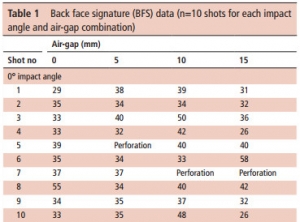
Armour panels representative of typical police armour (400x400 mm) were mounted on calibrated Roma Plastilina No 1 and impacted with 9 mm Luger FMJ (9×19 mm; full metal jacket; Dynamit Nobel DM11A1B2) ammunition at 365±10 m/s with a range of air-gaps(0-15 mm). Whether or not the ammunition perforated the armour was noted, the BFS was measured and the incidence of pencilling (a severe, deep and narrow BFS) was identified.
RESULTS:
For 0° impacts, a critical air-gap size of 10 mm is detrimental to armour performance for the armour/ammunition combination assessed in this work. Specifically, the incidences of pencilling were more common with a 10 mm air-gap and resulted in BFS depth:volume ratios ≥1.0. For impacts at 30° the armour was susceptible to perforation irrespective of air-gap.
CONCLUSIONS:
This work suggested that an air-gap behind police body armour might result in an increased likelihood of injury. It is recommended that body armour is worn with no air-gap underneath.
14/11/2017
Balles en caoutchouc: Pas si anodines !
------------------------------
Cet article ne fait que confirmer le fait que certaines munitions en caoutchouc sont dangereuses (1) voire mortelles (2). Les lésions rapportées sont ici périphériques mais tout peut se voir: Atteintes faciales (3);oculaires (4), thoraciques (5), crâniennes (6), vasculaires (7). Evidemment cela dépend du type de munitions employées qui sont d'une grande variété.
------------------------------
Rubber bullets are considered a non-lethal method of crowd control and are being used over the world. However the literature regarding the pattern and management of these injuries is scarce for the forensic pathologist as well as for the traumatologist. The objective of this report was to add our experience to the existing literature.
METHODS:
From June 2008 to August 2010 the Government Hospital for Bone and Joint Surgery Barzulla and the Department of Orthopaedics, SKIMS Medical College/Hospital Bemina Srinagar received 28 patients for management of their orthopaedic injuries caused by rubber bullets. We documented all injuries and also recorded the management issues and complications that we encountered.
RESULTS:
All patients weremales with an age range of 11-32 years and were civilians who had been hit by rubber bullets fired by the police and the paramilitary forces. Among them, 19 patients had injuries of the lower limbs and 9 patients had injuries of the upper limbs. All patients were received within 6 h of being shot.
CONCLUSION:
Our findings suggest that these weapons are capable of causing significant injuries including fractures and it is important for the surgeon to be well versed with the management of such injuries especially in areas of unrest. The report is also supportive of the opinion that these weapons are lethal and should hence be reclassified.
30/06/2017
Trauma sonore: Protection et corticoïdes
Acute Acoustic Trauma among Soldiers during an Intense Combat.
-----------------------------------
BACKGROUND:
During military actions, soldiers are constantly exposed to various forms of potentially harmful noises. Acute acoustic trauma (AAT) results from an impact, unexpected intense noise ≥140 dB, which generates a high-energy sound wave that can damage the auditory system.
PURPOSE:
We sought to characterize AAT injuries among military personnel during operation "Protective Edge," to analyze the effectiveness of hearing protection devices (HPDs), and to evaluate the benefit of steroid treatment in early-diagnosed AAT injury.
RESEARCH DESIGN:
We retrospectively identified affected individuals who presented to military medical facilities with solitary or combined AAT injuries within 4 mo following an intense military operation, which was characterized with an abrupt, intensive noise exposure (July-December 2014).
STUDY SAMPLE:
A total of 186 participants who were referred during and shortly after a military operation with suspected AAT injury.
INTERVENTIONS:
HPDs, oral steroids.
DATA COLLECTION AND ANALYSIS:
Data extracted from charts and audiograms included demographics, AAT severity, worn HPDs, first and last audiograms and treatment (if given). The Student's independent samples t test was used to compare continuous variables. All tests were considered significant if p values were ≤0.05.
RESULTS:
A total of 186 participants presented with hearing complaints attributed to AAT: 122, 39, and 25 were in duty service, career personnel, and reservists, with a mean age of 21.1, 29.2, and 30.4 yr, respectively. Of them, 92 (49%) participants had confirmed hearing loss in at least one ear. Hearing impairment was significantly more common in unprotected participants, when compared with protected participants: 62% (74/119) versus 45% (30/67), p < 0.05. Tinnitus was more common in unprotected participants when compared with protected participants (75% versus 49%, p = 0.04), whereas vertigo was an uncommon symptom (5% versus 2.5%, respectively, p > 0.05). In the 21 participants who received steroid treatment for early-diagnosed AAT, bone-conduction hearing thresholds significantly improved in the posttreatment audiograms, when compared with untreated participants (p < 0.01, for 1-4 kHz).
CONCLUSIONS:
AAT is a common military injury, and should be diagnosed early to minimize associated morbidity. HPDs were proven to be effective in preventing and minimizing AAT hearing sequelae. Steroid treatment was effective in AAT injury, if initiated within 7 days after noise exposure.
| Tags : blast
10/03/2017
Sauvetage au combat à la mer: Quid ?
Multi-Injury Casualty Stream Simulation in a Shipboard Combat Environment
-------------------------
L'attention portée à la prise en charge des blessés de guerre se porte essentiellement aux blessés lors de combat se déroulant au sol. Il ne faut pas oublier aussi ce qui se passe sur (voire sous) la surface de la mer. Ce qui est vrai à terre ne l'est probablement pas à la mer. Le trauma des membres est certainement moins prééminent. Les mécanismes ballistiques, l'environnement de prise en charge sont totalement différents aussi les réponses, c'est à dire la manière de conduire le sauvetage au combat, le sont également. Cependant la rareté des engagements sur mer rend difficile la mise sur pied d'une conduite basée sur les faits, d'où l'intérêt des outils de simulation statistique. C'est ce que propose cet article.
-------------------------
| Trauma Category | AIREX(%) | UNDEX(%) |
| Amputations (a) | 3.00 | 3.00 |
| Asphyxiations | 1.34 | 3.50 |
| Burns | 25.30 | 15.09 |
| Concussions/Internal Organs | 2.85 | 9.29 |
| Contusions/Abrasions | 7.06 | 16.28 |
| Fractures | 6.70 | 11.52 |
| Miscellaneous | 4.96 | 12.08 |
| Nonfatal Immersions | 2.00 | 2.00 |
| Penetrating Wounds | 44.88 | 20.49 |
| Sprains/Strains/Dislocations | 1.91 | 6.75 |
| Total | 100.00 | 100.00 |
| Tags : naval
10/12/2016
Tueries massives par armes à feu: Penser différemment !
The profile of wounding in civilian public mass shooting fatalities.
BACKGROUND:
The incidence and severity of civilian public mass shootings (CPMS) continue to r.ise. Initiatives predicated on lessons learned from military woundings have placed strong emphasis on hemorrhage control, especially via use of tourniquets, as means to improve survival. We hypothesize that both the overall wounding pattern and the specific fatal wounds in CPMS events are different from those in military combat fatalities and thus may require a new management strategy.
METHODS:
A retrospective study of autopsy reports for all victims involved in 12 CPMS events was performed. Civilian public mass shootings was defined using the FBI and the Congressional Research Service definition. The site of injury, probable site of fatal injury, and presence of potentially survivable injury (defined as survival if prehospital care is provided within 10 minutes and trauma center care within 60 minutes of injury) was determined independently by each author.
RESULTS:
A total 139 fatalities consisting of 371 wounds from 12 CPMS events were reviewed. All wounds were due to gunshots. Victims had an average of 2.7 gunshots. Relative to military reports, the case fatality rate was significantly higher, and incidence of potentially survivable injuries was significantly lower. Overall, 58% of victims had gunshots to the head and chest, and only 20% had extremity wounds. The probable site of fatal wounding was the head or chest in 77% of cases.
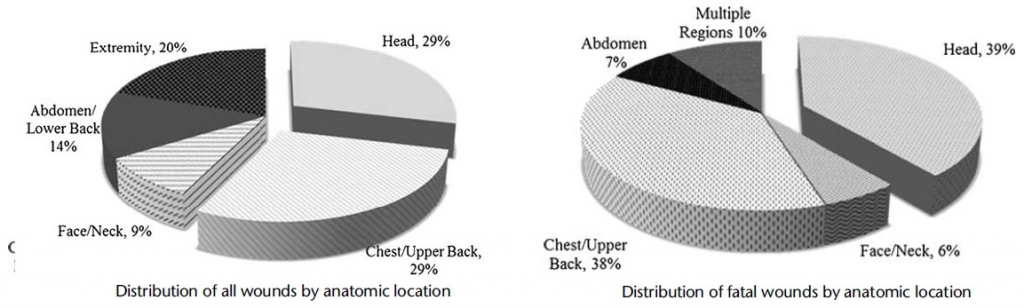
Only 7% of victims had potentially survivable wounds. The most common site of potentially survivable injury was the chest (89%). No head injury was potentially survivable. There were no deaths due to exsanguination from an extremity.
CONCLUSION:
The overall and fatal wounding patterns following CPMS are different from those resulting from combat operations. Given that no deaths were due to extremity hemorrhage, a treatment strategy that goes beyond use of tourniquets is needed to rescue the few victims with potentially survivable injuries.
10/11/2016
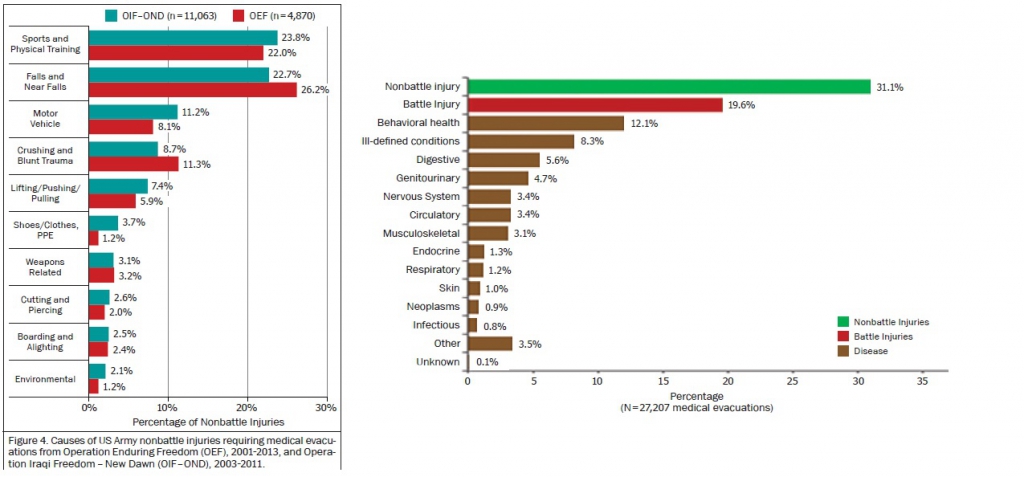
Evasan: Surtout des blessés non en rapport avec la guerre
Surveillance of Disease and Nonbattle Injuries During US Army Operations in Afghanistan and Iraq.
Hauret KG et Al. US Army Med Dep J. 2016 Apr-Sep;(2-16):15-23.
Disease and nonbattle injury (DNBI) are the leading causes of morbidity during wars and military operations. However, adequate medical data were never before available to service public health centers to conduct DNBI surveillance during deployments. This article describes the process, results and lessons learned from centralized DNBI surveillance by the US Army Center for Health Promotion and Preventive Medicine, predecessor of the US Army Public Health Command, during operations in Afghanistan and Iraq (2001-2013).The surveillance relied primarily on medical evacuation records and in-theater hospitalization records. Medical evacuation rates (per 1,000 person-years) for DNBI were higher (Afghanistan: 56.7; Iraq: 40.2) than battle injury rates (Afghanistan: 12.0; Iraq: 7.7). In Afghanistan and Iraq, respectively, the leading diagnostic categories for medical evacuations were nonbattle injury (31% and 34%), battle injury (20% and 16%), and behavioral health (12% and 10%). Leading causes of medically evacuated nonbattle injuries were sports/physical training (22% and 24%), falls (23% and 26%) and military vehicle accidents (8% and 11%).
This surveillance demonstrated the feasibility, utility, and benefits of centralized DNBI surveillance during military operations.