26/10/2017
Afflux massif: Que fait on vraiment ?
Prehospital Interventions During Mass-Casualty Events in Afghanistan: A Case Analysis.
BACKGROUND:
Mass-casualty (MASCAL) events are known to occur in the combat setting. There are very limited data at this time from the Joint Theater (Iraq and Afghanistan) wars specific to MASCAL events. The purpose of this report was to provide preliminary data for the development of prehospital planning and guidelines.
METHODS:
Cases were identified using the Department of Defense (DoD; Virginia USA) Trauma Registry (DoDTR) and the Prehospital Trauma Registry (PHTR). These cases were identified as part of a research study evaluating Tactical Combat Casualty Care (TCCC) guidelines. Cases that were designated as or associated with denoted MASCAL events were included. Data Fifty subjects were identified during the course of this project. Explosives were the most common cause of injuries. There was a wide range of vital signs. Tourniquet placement and pressure dressings were the most common interventions, followed by analgesia administration.
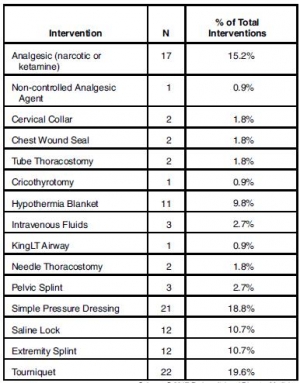
Oral transmucosal fentanyl citrate (OTFC) was the most common parenteral analgesic drug administered. Most were evacuated as "routine." Follow-up data were available for 36 of the subjects and 97% were discharged alive.
CONCLUSIONS:
The most common prehospital interventions were tourniquet and pressure dressing hemorrhage control, along with pain medication administration. Larger data sets are needed to guide development of MASCAL in-theater clinical practice guidelines.
| Tags : mascal
21/10/2017
Serious game ? Peut-être mais pas sûr
- ---------------------------------------------------
AIM:
In modern warfare, almost 25% of combat-related deaths are considered preventable if life-saving interventions are performed. Therefore, Tactical Combat Casualty Care (TCCC) training for soldiers is a major challenge. In 2014, the French Military Medical Service supported the development of 3D-SC1®, a serious game designed for the French TCCC program, entitled Sauvetage au Combat de niveau 1 (SC1). Our study aimed to evaluate the impact on performance of additional training with 3D-SC1®.
MATERIAL AND METHODS:
The study assessed the performance of soldiers randomly assigned to one of two groups, before (measure 1) and after (measure 2) receiving additional training. This training involved either 3D-SC1® (Intervention group), or a DVD (Control group). The principal measure was the individual performance (on a 16-point scale), assessed by two investigators during a hands-on simulation. First, the mean performance score was compared between the two measures for Intervention and Control groups using a two-tailed paired t-test. Second, a multivariable linear regression was used to determine the difference in the impacts of 3D-SC1® and DVD training, and the order of presentation of the two scenarios, on the mean change from baseline in performance scores.
RESULTS AND DISCUSSION:
A total of 96 subjects were evaluated: seven could not be followed-up, while 50 were randomly allocated to the Intervention group, and 39 to the Control group. Between measure 1 and measure 2, the mean (SD) performance score increased from 9.9 (3.13) to 14.1 (1.23), and from 9.4 (2.97) to 12.5 (1.83), for the Intervention group and Control group, respectively (p<0.0001). The adjusted mean difference in performance scores between 3D-SC1® and DVD training was 1.1 (95% confidence interval -0.3, 2.5) (p=0.14). Overall, the study found that supplementing SC1 training with either 3D-SC1® or DVD improved performance, assessed by a hands-on simulation. However, our analysis did not find a statistically significant difference between the effects of these two training tools. 3D-SC1® could be an efficient and pedagogical tool to train soldiers in life-saving interventions. In the current context of terrorist threat, a specifically-adapted version of 3D-SC1®may be a cost-effective and engaging way to train a large civilian public.
18/10/2017
On peut rêver

Philippe Chapleau nous apprend que dans le cadre de son déploiement en Europe, les 1900 soldats de la 1st Air Cavalry Brigade disposera disposeront de 12 Chinook, 38 Black Hawk, 24 Apache et 15 Black Hawk médicalisés. On peut rêver.
| Tags : medevac
15/10/2017
RFE 2017 In/Extubation en anesthésie
Clic sur l'image pour accéder au document
| Tags : intubation, coniotomie, airway
14/10/2017
TCCC Quick Reference Guide

Clic sur l'image pour accéder au document
| Tags : tccc
12/10/2017
Perception des Médecins par les militaires
Clic sur l'image pour accéder au document
Chirurgie Pédiatrique en opex
Clic sur l'image pour accéder au document
Activité d'urgence en role 3 à Kaboul
Clic sur l'image pour accéder au document
11/10/2017
Le site du CARUM

Clic sur l'image pour accéder au lien
| Tags : carum
Numéro Spécial SSA

Clic sur l'image pour accéder au sommaire
01/10/2017
Exsufflation axillaire: Plus sûre
Relative device stability of anterior versus axillary needle decompression for tension pneumothorax during casualty movement: Preliminary analysis of a human cadaver model
BACKGROUND:
Tension pneumothorax (tPTX) remains a significant cause of potentially preventable death in military and civilian settings. The current prehospital standard of care for tPTX is immediate decompression with a 14-gauge 8-cm angiocatheter; however, failure rates may be as high as 17% to 60%. Alternative devices, such as 10-gauge angiocatheter, modified Veress needle, and laparoscopic trocar, have shown to be potentially more effective in animal models; however, little is known about the relative insertional safety or mechanical stability during casualty movement.
METHODS:
Seven soft-embalmed cadavers were intubated and mechanically ventilated. Chest wall thickness was measured at the second intercostal space at the midclavicular line (2MCL) and the fifth intercostal space along the anterior axillary line (5AAL). CO2 insufflation created a PTX, and needle decompression was then performed with a randomized device. Insertional depth was measured between hub and skin before and after simulated casualty transport. Thoracoscopy was used to evaluate for intrapleural placement and/or injury during insertion and after movement. Cadaver demographics, device displacement, device dislodgment, and injuries were recorded. Three decompressions were performed at each site (2MCL/5AAL), totaling 12 events per cadaver.
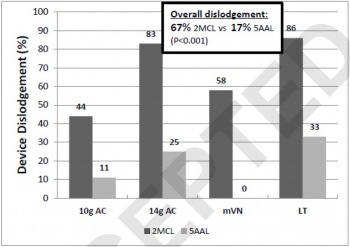
RESULTS:
Eighty-four decompressions were performed. Average cadaver age was 59 years, and body mass index was 24 kg/m. The CWT varied between cadavers because of subcutaneous emphysema, but the average was 39 mm at the 2MCL and 31 mm at the 5AAL. Following movement, the 2MCL site was more likely to become dislodged than the 5AAL (67% vs. 17%, p = 0.001). Median displacement also differed between 2MCL and 5AAL (23 vs. 2 mm, p = 0.001). No significant differences were noted in dislodgement or displacement between devices. Five minor lung injuries were noted at the 5AAL position.
CONCLUSION:
Preliminary results from this human cadaver study suggest the 5AAL position is a more stable and reliable location for thoracic decompression of tPTX during combat casualty transport.
| Tags : pneumothorax
Bon usage pharmaceutique en OPEX