24/04/2015
Pneumothorax: Passez par le côté
Failed needle decompression of bilateral spontaneous tension pneumothorax
Bac PT et Al. Acta Anaesthesiol Scand. 2015 Apr 21. doi: 10.1111/aas.12538. [Epub ahead of print]
-------------------------------------------------
Cet article a le mérite de rappeler que la détresse respiratoire est ua prmeier plan enc as de pneumothorax suffocant chez le patient non ventilé, que la voie latérale doit être privilégié et surtout que la thoracostomie simple est parfaitement efficace.
-------------------------------------------------
This case report presents a young male admitted with primary bilateral spontaneous tension pneumothorax and severe respiratory distress. This is an extremely rare condition. The patient was on the verge of hypoxic cardiac arrest and the attempted needle thoracocentesis was unsuccessful. Needle thoracocentesis in the midclavicular line of the second intercostal space is widely used and recommended as first-line treatment of tension pneumothorax. Reviewing the literature, the procedure is not based on solid evidence. It has high failure rates and potentially serious complications. Alternatives to this approach are perhaps more appropriate. Correctly done, needle thoracocentesis has its place in the presence of a diagnosed or suspected tension pneumothorax when no other options are available. If needle thoracocentesis is chosen, then insertion in the mid-anterior axillary line of the 3rd–5th intercostal space is an appropriate alternative site. Otherwise, lateral thoracostomy, with or without chest tube insertion, is a safe procedure with a high success rate. It should be considered as the first-line treatment of tension pneumothorax, particularly in the unstable patient
| Tags : pneumothorax, exsufflation
06/04/2015
Soins obstétricaux Manuel MSF
| Tags : obstétrique
04/04/2015
Simulateur de tâche: Modifié pour + de réalisme!
Rescuing the obese or burned airway: are conventional training manikins adequate? A simulation study
Howes TE. et Al. Br J Anaesth. 2015 Jan;114(1):136-42
-------------------------------------------------
L'emploi de simulateurs de taches se heurte au problème du réalisme de ces derniers. Cette équipe propose de modifier les simulateurs industriels pour plus de réalité.
-------------------------------------------------
Background. Percutaneous tracheal access is required in more than 40% of major airway emergencies, and rates of failure are high among anaesthetists. Supraglottic airway management is more likely to fail in patients with obesity or neck pathology. Commercially available manikins may aid training. In this study, we modified a standard ‘front of neck’ manikin and evaluated anaesthetists’ performance of percutaneous tracheal access.
Methods. Two cricothyroidotomy training manikins were modified using sections of belly pork to simulate a morbidly obese patient and an obese patient with neck burns.

An unmodified manikin was used to simulate a slim patient. Twenty consultant anaesthetists were asked to manage a ‘can’t intubate, can’t ventilate’ scenario involving each of the three manikins. Outcome measures were success using their chosen technique and time to first effective breath.
Results. Success rates using first-choice equipment were: ‘slim’ manikin 100%, ‘morbidly obese’ manikin 60%, and ‘burned obese’ manikin 77%. All attempts on the ‘slim’ manikin succeeded within 240 s, the majority within 120 s. In attempts on the ‘morbidly obese’ manikin, 60% succeeded within 240 s and 20% required more than 720 s. All attempts on the ‘burned obese’ manikin succeeded within 180 s.
Conclusions. Significantly greater technical difficulty was experienced with our ‘morbidly obese’ manikin compared with the unmodified manikin. Failure rates and times to completion were considerably more consistent with real-life reports. Modifying a standard manikin to simulate an obese patient is likely to better prepare anaesthetists for this challenging situation. Development of a commercial manikin with such properties would be of value
| Tags : coniotomie
Crico: S'entraîner sur un modèle animal est pertinent ?
Comparison of manikin versus porcine models in cricothyrotomy procedure training
Cho J et Coll. Emerg Med J 2008;25:732-734
--------------------------------------------------------------------------
Le choix du simulateur de tache utilisé pour l'enseignement de la coniotomie reste une vrai question. Modèle humain, animal ou artificiel. Cet article met en avant l'intérêt du modèle animal qui offrirait plus de réalité anatomique. Néanmoins il faut lire ce document avec un peu de recul car la coniotomie est un geste peu fréquemment réalisé, et probablement que la notion de réalisme porte plutôt sur les aspects anatomiques de la région cervicale que sur le réalisme de pratique de geste sur la région cervicale. Encore faut-il pouvoir dans la vrai vie pouvoir disposer d'une filière d'approvisionnement qui souvent se résume au boucher du quartier.
--------------------------------------------------------------------------
Objective: To compare the usefulness for training of a porcine model (larynx, trachea, and pig skin) and a manikin model using a Portex cricothyrotomy kit (PCK).
Methods: In a prospective randomised crossover trial, participants in the airway workshop performed crico-thyrotomy using a PCK on the porcine and manikin models (Tracheostomy Trainer and Case). The porcine model was made with larynxes and trachea from freshly slaughtered pigs and covered with a piece of thinned pigskin stapled to a wooden board.
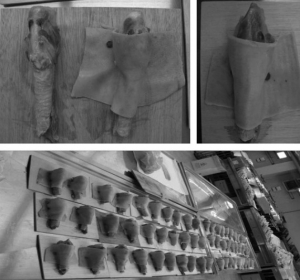
Participants were asked to assess the following: reality of skin turgor; difficulty with skin penetration, landmark recognition and procedure; reality of the model; and preference for each model using a visual analogue scale (VAS) of 0–10 cm. The VAS scores for each model were compared.
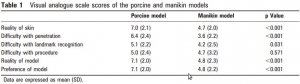
Results: 49 participants were included in the study. Mean (SD) VAS scores for the reality of skin turgor, degree of difficulty with skin penetration and landmark recognition were higher with the porcine model than with the manikin model (7.0 (2.1) vs 4.7 (2.0), 6.4 (2.4) vs 3.6 (2.2), 5.1 (2.2) vs 4.2 (2.5), respectively). There was no difference between the models in the difficulty of the procedure (5.0 (2.4) vs 4.7 (3.2)). The porcine model had a higher VAS score for overall reality and preference of the model (7.1 (2.0) vs 4.8 (2.3) and 7.1 (2.0) vs 4.8 (2.2), respectively).
Conclusion: The porcine model is a more useful training tool than the manikin model for cricothyrotomy with PCK because of its reality and similarity to human anatomy.
| Tags : coniotomie
Crico: Pour en savoir plus en 5 min ?
Large-bore cricothyroidotomy devices
Patel B. et Al. Contin Educ Anaesth Crit Care Pain(2008) 8 (5): 157-160
L'article proposé fait une revue simple des divers équipements permettant la réalisation d'une coniotomie. Il apporte par ailleurs quelques compléments d'informations sur les facteurs de réussite de cette pratique dont l'éventualité d'occurrence est faible mais à laquelle il faut se préparer.
| Tags : coniotomie
Simulateur de crico: Encore le modèle porcin
A home-made animal model in comparison with a standard manikin for teaching percutaneous dilatational tracheostomy
Interact Cardiovasc Thorac Surg. 2015 Feb;20(2):248-53

| Tags : coniotomie, simulateurs
03/04/2015
Echographiste en quelques heures ?
Limited intervention improves technical skill in focus assessed transthoracic echocardiography among novice examiners.
Frederiksen et al. BMC Med Educ. 2012 Aug 3;12:65
-------------------------------------------------------------------
La généralisation de l'échographie est une avancée majeure. Mais comment apprendre ? La pratique de l'échographie ciblée se développe notamment en médecine d'urgence. A côté des formations classiques de type DU existent de nombreuses formations de courte durée, certaines de quelques heures. Le travail présenté met en évidence qu'un tel type de formation permet une manipulation relativement fiable des équipements et l'obtention de coupes sonographiques propres à être interprétées. On notera que ceci est obtenu A CONDITION qu'au moins 10 examens supervisés soient conduits, ce qui n'est souvent pas fait avec suffisamment de rigueur dans ce que nous pouvons proposer actuellement. Par ailleurs voir et interpréter de manière fiable ne sont pas superposables (1).
-------------------------------------------------------------------
BACKGROUNDS:
Previous studies addressing teaching and learning in point-of-care ultrasound have primarily focussed on image interpretation and not on the technical quality of the images. We hypothesized that a limited intervention of 10 supervised examinations would improve the technical skills in Focus Assessed Transthoracic Echocardiography (FATE) and that physicians with no experience in FATE would quickly adopt technical skills allowing for image quality suitable for interpretation.
METHODS:
Twenty-one physicians with no previous training in FATE or echocardiography (Novices) participated in the study and a reference group of three examiners with more than 10 years of experience in echocardiography (Experts) was included. Novices received an initial theoretical and practical introduction (2 hours), after which baseline examinations were performed on two healthy volunteers. Subsequently all physicians were scheduled to a separate intervention day comprising ten supervised FATE examinations. For effect measurement a second examination (evaluation) of the same two healthy volunteers from the baseline examination was performed.
RESULTS:
At baseline 86% of images obtained by novices were suitable for interpretation, on evaluation this was 93% (p = 0.005). 100% of images obtained by experts were suitable for interpretation. Mean global image rating on baseline examinations was 70.2 (CI 68.0-72.4) and mean global image rating after intervention was 75.0 (CI 72.9-77.0), p = 0.0002. In comparison, mean global image rating in the expert group was 89.8 (CI 88.8-90.9).
CONCLUSIONS:
Improvement of technical skills in FATE can be achieved with a limited intervention and upon completion of intervention 93% of images achieved are suitable for clinical interpretation.
| Tags : échographie