25/11/2014
Dermatologie d'altitude: La connnaître
Incidence and Care of Environmental Dermatoses in the High-Altitude Region of Ladakh, India
Singh GK et All. Indian J Dermatol. 2013 Mar-Apr; 58(2): 107–112.
BACKGROUND:
Low humidity, high-velocity wind, excessive ultraviolet (UV) exposure, and extreme cold temperature are the main causes of various types of environmental dermatoses in high altitudes.
MATERIALS AND METHODS:
A retrospective study was carried out in patients visiting the lone dermatology department in Ladakh between July 2009 and June 2010. The aim was to identify the common environmental dermatoses in high altitudes so that they can be treated easily or prevented. The patients were divided into three demographic groups, namely, lowlanders, Ladakhis (native highlanders), and tourists. Data was analyzed in a tabulated fashion.
RESULTS:
A total of 1,567 patients with skin ailments were seen, of whom 965 were lowlanders, 512 native Ladakhis, and 90 were tourists. The skin disorders due to UV rays, dry skin, and papular urticaria were common among all groups. The frequency of melasma (n = 42; 49.4%), chronic actinic dermatitis (CAD) (n = 18; 81.81% of total CAD cases), and actinic cheilitis (n = 3; 100%) was much higher among the native Ladakhis. The frequency of cold-related injuries was much lesser among Ladakhis (n = 1; 1.19%) than lowlanders (n = 70; 83.33%) and tourists (n = 13; 15.47%) (P < 0.05).
CONCLUSION:
Dryness of skin, tanning, acute or chronic sunburn, polymorphic light reaction, CAD, insect bite reactions, chilblain, and frostbite are common environmental dermatoses of high altitudes. Avoidance of frequent application of soap, application of adequate and suitable emollient, use of effective sunscreen, and wearing of protective clothing are important guidelines for skin care in this region.
| Tags : altitude
12/11/2014
Prevention and Treatment of Acute Altitude Illness
Wilderness Medical Society Consensus Guidelines for the Prevention and Treatment of Acute Altitude Illness
Luks AM et All. Wilderness Environ Med. 2010 Jun;21(2):146-55
To provide guidance to clinicians about best practices, the Wilderness Medical Society (WMS) convened an expert panel to develop evidence-based guidelines for the prevention and treatment of acute mountain sickness (AMS), high altitude cerebral edema (HACE), and high altitude pulmonary edema (HAPE). These guidelines present the main prophylactic and therapeutic modalities for each disorder and provide recommendations for their roles in disease management. Recommendations are graded based on the quality of supporting evidence and balance between the benefits and risks/burdens according to criteria put forth by the American College of Chest Physicians. The guidelines also provide suggested approaches to the prevention and management of each disorder that incorporate these recommendations.
| Tags : altitude
Hypothermie accidentelle: Guidelines 2014 de la WMS
Wilderness Medical Society Practice Guidelines for the Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia
Zaphren K. et All. Wilderness Environ Med. 2014 in press
----------------------------------------------------
Doit être remarqué la recommandation de ne pas mobiliser le blessé hypotherme pendant au moins 30 min après la mise en oeuvre des techniques de réchauffement. Ceci a pour objet de limiter les effets de l'afterdrop, mécanisme par lequel le réchauffement peut transitoirement aggraver l'hypothermie centrale par un mécanisme de recirculation de sang froid.
----------------------------------------------------

1. The key factors to guide treatment are level of consciousness, shivering intensity, and cardiovascular stability, based on blood pressure and cardiac rhythm Core temperature can provide additional helpful information (panel consensus).
2. A patient who is shivering but able to function well and to care for himself or herself is unlikely to be hypothermic. A patient who is shivering, becoming incapacitated, and having difficulty caring for himself or herself is likely to be hypothermic. If there is any doubt, assume that the patient is hypothermic (panel consensus).
3. Because the temperature ranges to which the HT grades are meant to correspond are the same as the standard classification, rescuers should refer to mild, moderate, severe, and profound hypothermia (<24°C) on the basis of their clinical observations, remembering that shivering can occur below 32°C, usually with altered mental status, and that patients can have detectable vital signs with core temperatures below 24°C (panel consensus).
4. Clinicians should consider causes other than hypothermia to explain altered mental status or lack of shivering that does not correlate with the measured core temperature or by a history of minimal cold exposure (panel consensus).
5. In a patient whose airway has been secured with an endotracheal tube or with a supraglottic airway that has a port for placing a gastric tube, use esophageal temperature monitoring with the esophageal temperature probe inserted into the lower third of the esophagus (1C).
6. Use an epitympanic thermometer designed for field conditions with an isolating ear cap in a patient whose airway has not been secured by endotracheal intubation or a supraglottic airway or in a patient with a secured airway if an esophageal probe is not available (1C)
7. Rectal temperature should not be measured in the field until the patient is in a warm environment (1C).
8.Use oral temperature measurement with a thermometer (electronic or liquid-filled) that can read below 35°C only to rule out hypothermia (1A).
9. Monitor rectal or bladder temperature during rewarming of an unconscious patient only if an esophageal or epitympanic probe is not available. If rectal or bladder temperature is used for monitoring during rewarming, allow for inaccuracy owing to the time lag behind core temperature changes (1A).
10. Do not use a temporal artery thermometer in a possibly hypothermic patient (1C)
11. The decision to rescue or to resuscitate a potentially severely hypothermic patient should only be made after the scene is secure and safe for the rescuers to enter and make an evaluation (1A). After safety of rescuers has been assured, the priorities in out-of-hospital treatment of a hypothermic patient who is not in cardiac arrest are to avoid causing cardiovascular collapse during rescue, to prevent a further decrease in core temperature (afterdrop), and to rewarm the patient in a safe manner. If a hypothermic patient is in cardiac arrest, rescuers should initiate resuscitation, if indicated.
12. Rescuers should keep a hypothermic patient horizontal, especially during rescue from water or from a crevasse (1B) and should limit physical effort by the patient during rescue (1B). A conscious patient should be encouraged to be vigilant and focus on survival (1C).
13. Handle a hypothermic patient gently and continue to keep the patient horizontal (1B). Avoid any disturbance, especially movement of the extremities that might precipitate VF (1B). Once the patient is in a warm environment, clothes should be cut off rather than removed manually (1B)
14. Protect from further cooling by using insulation and a vapor barrier until the patient has reached a warm environment, such as the interior of an ambulance. Remove wet clothes, preferably by cutting them off, only when the patient has been protected from the cold (1C). Take special care to insulate the patient from the ground (eg, with sleeping pads) to protect from conductive heat loss and also to protect the head and neck by closing the area around the face as effectively as possible (1C).
15. Use an outer windproof layer to protect the patient from wind and especially from rotor wash when loading or unloading from a helicopter (1C).
16. Shivering is an effective method of rewarming a patient who is cold but not hypothermic or who is mildly hypothermic. The patient must have sufficient energy reserves to sustain shivering and must be adequately insulated from the environment to retain the heat that is generated (1A)
17. An alert patient who is shivering, and who is not at risk for aspiration, should receive high-carbohydrate liquids and food. Liquids and food may be warmed but should not be hot enough to cause burns (1C).
18. Initially, a hypothermic patient should not be allowed to stand or walk (1C)
19. A shivering patient who may be hypothermic should be kept as warm as possible, given calorie replacement, and observed for at least 30 minutes before exercising. The patient should be monitored closely. An alert patient may be allowed to stand. If the patient can stand without difficulty, exercise intensity should start low and increase gradually as tolerated (1C)
20. Large heat pads should be used, if available (1B). Rewarming devices should be used in conjunction with vapor barriers and insulation (1C). The HeatPac should only be used outdoors or with proper ventilation that is carefully monitored (1B).
21. Body-to-body rewarming can be used in mild hypothermia to increase patient thermal comfort if enough personnel are available and if it does not delay evacuation to definitive care (1B).
22. Apply heat sources to the axillae, chest, and back. A large heat pad or blanket should be placed over the chest and, if large enough, extended into the axillae and under the back (1B). Additional heat, if available, can be applied to the neck if precautions are taken to prevent heat loss through any neck opening (1C). Avoid applying external heat to the extremities, although it is not necessary to insulate the arms from heat applied to the torso (1B).
23. The HPMK can be used as a convenient and effective means of preventing heat loss and providing active external rewarming (1C).
24. Avoid localized pressure to cold skin. Heat should never be applied directly to the skin. A barrier should be used to prevent burning the skin when using chemical or electrical heat pads or warm water bottles (1C).
25. Do not use small chemical heat packs for rewarming a hypothermic patient (1B). Small chemical heat packs can be used to prevent local cold injury to the hands and feet during treatment and transport (1C).
26. Heated humidified oxygen can be used in combination with other rewarming methods (2C), but should not be relied on as the only rewarming method (1B).
27. Do not use a warm shower or bath for rewarming, even if a patient appears to be only mildly hypothermic (1C).
28. Distal limb warming to the elbows and knees in 421C to 451C water can be used for rewarming a patient with mild hypothermia (1C).
29. Forced-air warming should be used during air or ground transport, if available (1A). If forced-air warming is not available, use of heat pads, including the HPMK, can be continued. Care must be take to prevent CO buildup with the charcoal HeatPac in a ground ambulance; this can be done by igniting the device outside the vehicle, bringing it inside only after initial smoke production subsides, ventilating the vehicle compartment, and monitoring CO (1C). HeatPac should not be used in an aircraft (1C).
30. Patient compartments in ground and air ambulances should be heated to at least 241C, if possible, to decrease further heat loss (1C).
31. A cold-stressed patient who is not hypothermic does not need to be kept horizontal. The patient may be allowed to remove his or her own wet clothing and to put on dry clothing without shelter, if necessary. The patient may be allowed to rest in a sitting position, to eat and drink to maintain energy reserves and hydration, and may move or keep moving, if necessary (panel consensus).
32. Fixed, dilated pupils, apparent rigor mortis, and dependent lividity are not contraindications to resuscitation of a severely hypothermic patient (1A for fixed, dilated pupils and apparent rigor mortis; 2C for dependent lividity). If there are no contraindications to cardiopulmonary resuscitation (CPR), rescuers should not give up hope and should attempt resuscitation (1A).
33. Do not attempt to resuscitate a patient with obvious fatal injuries or whose chest wall is too stiff for compressions (1A).
34. Do not attempt resuscitation in an avalanche victim buried for 35 minutes or longer with an airway that is definitely obstructed by snow or ice (1A).
35. Rescuers should make every effort to move the patient to a warm setting, such as a ground or air ambulance or a medical facility where cardiac monitoring is available to guide resuscitation and to start rewarming (1C). Before starting CPR, feel for a carotid pulse for 1 minute. If there is no detectible pulse after 1 minute, start CPR, including rescue breathing (1C).
36. CPR should be started if a nonperfusing rhythm, including ventricular tachycardia (VT), VF, or asystole, is detected. If there is a cardiac rhythm with organized QRS complexes (other than VT), CPR should not be performed (1C) unless ETCO2 monitoring confirms lack of perfusion or echocardiography shows that there are no cardiac contractions corresponding to electrical activity (1B).
37. If shock is advised by the AED, attempt defibrillation and start CPR. If no shock is advised on an AED, no carotid pulse is found after palpating for at least 1 minute, normal breathing or other signs of life are not observed, and ultrasound is not available to verify cardiac activity or pulses, start CPR (1C).
38. In patients with severe or profound hypothermia, CPR can be delayed (“scoop and run”) and can be given intermittently during evacuation if it is not technically possible or safe to perform continuous CPR (1C). CPR can be given for several hours, if necessary (1B).
39. If there is no contraindication to CPR and no indication to terminate CPR, continue resuscitation attempts in a patient even if the core temperature is below 101C measured by an esophageal probe in the lower third of the esophagus (2C).
40. If a cardiac monitor is available, use maximal amplification to search for QRS complexes (1C).
41. If a monitor or defibrillator shows VT or VF or if shock is advised by an AED in a patient whose core temperature is thought to be below 301C, give a single shock at maximal power (1C).
42. Wait until a patient has been rewarmed at least 11C to 21C or to 301C before attempting further shocks (2C). Once the core temperature reaches 301C, follow defibrillation guidelines for normothermic patients (1C).
43. For cardiac arrest in a hypothermic patient, deliver chest compressions at the same rate as in normothermic patients (1C).
44. In the absence of ETCO2 monitoring, deliver ventilations at the same rate recommended for a normothermic patient,11,17 unless an advanced airway is in place (see below) (2C).
45. gement. Recommendation. In a patient with an advanced airway, if ETCO2 monitoring is not available, deliver ventilations at half the rate recommended for a normothermic patient to avoid hyperventilation (1C).
46. If ETCO2 monitoring is available, keep ETCO2 within the normal range. In rescues at altitudes above 1200 m, ALS personnel should be aware of the normal range of ETCO2 at a given altitude (1C).
47. High-quality CPR can be performed effectively during prolonged transport using a mechanical device (1C).
48. The advantages of advanced airway management outweigh the risk of causing VF (1C). A nasogastric or orogastric tube should also be placed to decompress the stomach, after the airway is secured (1C).
49. Below a core temperature of 301C, dosages of anesthetic and neuromuscular blocking agents should be lowered and intervals extended according to the degree of hypothermia. Current data are insufficient to recommend specific protocols (1C).
50. A hypothermic patient may receive supplemental oxygen, especially at altitudes greater than 2500 m. There is potential benefit and no known harm (1C).
51. If circulatory access cannot immediately be obtained with a peripheral IV catheter, access should be obtained by the IO method (1C). Central venous access can be obtained using a femoral line if no other option is available (1C).
52. Resuscitate a hypothermic patient with normal saline warmed to 401C to 421C given IV or IO. Use caution to prevent volume overload (1B).
53. When practical, fluids should be given as boluses rather than by continuous infusion (1C). The goal of fluid administration should be to maintain systolic blood pressure at a level that provides adequate perfusion, depending on the degree of hypothermia (1C).
54. Glucose should be administered to a hypothermic patient who is hypoglycemic (1A). Insulin is not initially indicated for hyperglycemia (1B). If glucose testing is not available, IV glucose can be administered empirically to a hypothermic patient with altered mental status (1C).
55. Transcutaneous pacing may be beneficial in hypothermia in the setting of bradycardia with hypotension disproportionate to the core temperature (2C).
56. No treatment is indicated for atrial dysrhythmias in a hemodynamically stable patient during rewarming (IB).
57. A severely injured patient should be treated early and aggressively with active rewarming during all phases of out-of-hospital care to prevent hypothermia (1B).
58. To prepare a patient for transport, potential spinal injuries should be stabilized105 (1C). Fractures and dislocations should be reduced as much as possible to normal anatomic configuration (1C). Open wounds should be covered (1C).
59. An uninjured patient who is completely alert and shivering may be treated without being transported to a hospital (1B).
60. If injuries meet trauma criteria, a patient should be transported to a trauma center (1B). An asphyxiated patient should be transported to a hospital for observation (1B).
61. A patient with moderate to severe hypothermia who is hemodynamically stable can be transferred to the closest hospital or other appropriate medical facility such as a rural clinic (1C). A patient who is hemodynamically unstable or who has a core temperature less than 281C should be transferred to a hospital capable of providing critical care and ECC, if possible. If this will require significant additional time—generally more than an additional hour—of non– critical care transport the patient should first be stabilized at a closer facility (1C). A patient in cardiac arrest should be transferred to a hospital capable of providing ECC if possible. If all other factors are equal, ECMO is preferable to CPB (1B). In geographic regions where there is no hospital capable of providing ECC or when a hospital capable of providing ECC is not accessible, transport a patient in cardiac arrest to the closest hospital where serum potassium can be measured and where resuscitation methods not involving ECC can be attempted for a patient whose serum potassium is 12 mmol/L or less. (Please see following section for use of biochemical markers.) (1C).
62. If an adult hypothermic patient has a potassium greater than 12 mmol/L, CPR should be terminated (1B).
63. An avalanche victim buried 35 minutes or less or with a core temperature of at least 321C should receive standard resuscitation, including CPR if in cardiac arrest67,120 (1C). If there is ROSC, the victim should be transported to the nearest hospital that can manage any associated injuries (1C). An avalanche victim who was buried more than 35 minutes or who has a core temperature less than 321C and has detectable vital signs should be transported to the nearest hospital or rural clinic for active rewarming (1C). If there are no vital signs and the airway is patent, CPR should be started67 (1B). An avalanche victim in cardiac arrest with an airway that is definitely obstructed should not be resuscitated if burial time was greater than 35 minutes or core temperature is less than 321C67 (1C). If there is any chance that the airway was patent, a short trial of CPR is warranted (1B).
64. An avalanche victim with CPR in progress should be transported to a hospital with the capability of performing extracorporeal rewarming if possible (1B). If it is not practical for the patient to go directly to a hospital that can perform extracorporeal rewarming and serum potassium has not already been measured, the patient should be transported to a hospital or clinic capable of measuring serum potassium (1C). Resuscitation should be continued only if serum potassium is 12 mmol/L or less (1B).
| Tags : hypothermie
05/11/2014
Heatpac: Ancien, oublié mais reste d'actualité
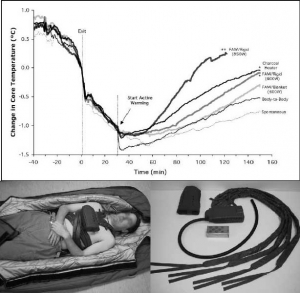
Pre-hospital torso-warming modalities for severe hypothermia: a comparative study using a human model
Objective: To compare 5 active torso-warming modalities in a human model of severe hypothermia with shivering heat production inhibited by intravenous meperidine.
Methods: Six subjects were cooled on 6 different occasions each, in 8°C water, for 30 minutes or to a core temperature of 35°C. Spontaneous warming was the first torso-warming modality to be tested for every subject, and results served both as a comparative control and for determination of the meperidine dose for subsequent trials. Meperidine (1.5 mg/kg) was administered during the final 10 minutes of immersion to suppress shivering. Subjects were removed from the water, dried and insulated for 30 minutes, followed by 120 minutes of 1) forced-air warming with either a 600-W heater and commercial soft warming blanket; or 2) a 600-W heater and rigid cover; or 3) an 850-W heater and rigid cover; or 4) a charcoal heater on the chest; or 5) direct body-to-body contact with a normothermic partner. Supplemental meperidine (to a maximum cumulative dose of 3.2 mg/kg) was administered as required to inhibit shivering.
Results: The initial post-cooling afterdrop was approximately 1.0°C. After 30 minutes, core temperature continued to drop by 0.45°C in spontaneous and body-to-body warming modalities. This post-warming afterdrop was significantly less with 600-W heater and rigid cover and the charcoal heater (0.26°C) and the least with 850-W heater and rigid cover (0.17°C). Core rewarming rates were highest using 850-W heater and rigid cover (1.45°C/hr), with charcoal heating and 600-W rigid heater (0.7°C/hr), 600-W heater and blanket (0.57°C/hr) and body-to-body warming (0.52°C/hr) being more effective than spontaneous warming (0.36°C/hr).
Conclusions: In non-shivering subjects, external heat application was effective in attenuating core temperature afterdrop and facilitating safe core rewarming; this was more evident when heat was delivered preferentially to the chest, and dependent upon the amount of heat donated. The modalities studied appear sufficiently practical and portable for pre-hospital use and should be considered for such situations, particularly in rural or wilderness locations where anticipated transport time to the hospital exceeds 30 minutes.
| Tags : hypothermie
04/11/2014
Gelures: L'expérience indienne
Management of Cold Injuries
Hota PK et Al. Surgical Research Updates, 2013, 1, 20-25
Un article produit par une équipe ayant une grande connaissance de cette pathologie. La place de l'oxygénothérapie hyperbare y est mise en avant.
____________________________________________________________
____________________________________________________________
| Tags : gelures
24/05/2014
Gelures: Une vision actualisée 2014
Frostbite: a practical approach to hospital management
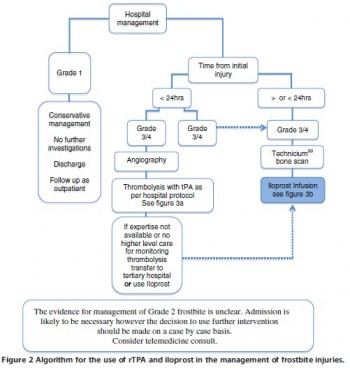
| Tags : gelures
16/01/2014
Coup de chaleur: Bases

| Tags : hyperthermie
15/01/2014
Coup de chaleur: Refroidir
Hyperthermie d’effort : comment refroidir ?
| Tags : hyperthermie
13/01/2014
Coup de chaleur: Explorer
Hyperthermie d’effort : pourquoi explorer ?
| Tags : hyperthermie
03/12/2013
Les gelures
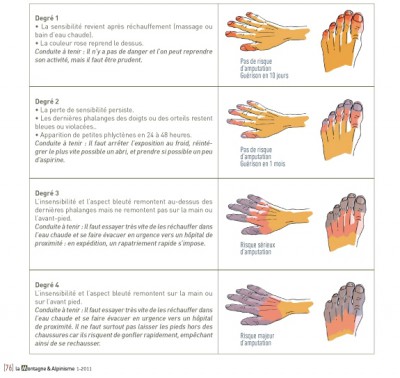
| Tags : gelures
Histoire de température
Clic sur l'image pour accéder au document
| Tags : hypothermie
01/12/2013
Cold weather: Epidémio US
Cold weather injuries, active and reserve components, U.S. Armed Forces, July 2008-June 2013.
Armed Forces Health Surveillance Center (AFHSC) MSMR. 2013 Oct;20(10):12-7
Hypothermie Engelures Gelures Pied de tranchée


Facteurs de risque: Jeune, de sexe féminin, ascendance africaine

Rate per 100,000 person-years
| Tags : hypothermie
23/11/2013
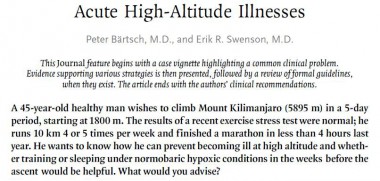
Hypothermie: Isoler étanche même mouillé est efficace !
Protection against Cold in Prehospital Care: Evaporative Heat Loss Reduction by Wet Clothing Removal or the Addition of a Vapor Barrier—A Thermal Manikin Study
Henriksson O. et Al. Prehosp Disaster Med 2012;26(6):1–6
Le travail présenté met en exergue les points suivants:
1. Le fait d'envelopper un organisme dans un contenant limite les pertes thermiques par évaporation .
2 Il est meilleur de multiplier les couches d'isolation.
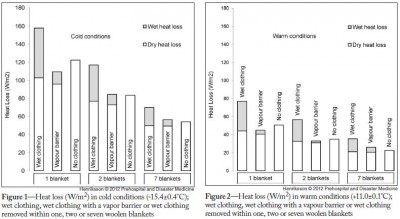
Il est fondamental que cet isolement soit parfaitement ETANCHE à l'air.
On rappelle que le principe de l'oignon (technique de hibbler)

1. La mise en place d'un écran interne au contact du blessé pour réduire les pertes thermiques par RADIATION (pertes thermiques par émission de rayonnement infrarouge, 50%des pertes) et par EVAPORATION (perte de calorie liée au changement d'état des molécules d'eau) (cutanée: 22 % des pertes et également respiratoire: 10 % des pertes) ainsi qu'en en protégeant les couches externes d'isolation de la transpiration et ou des défécations qui pourraient alors majorer les pertes par conduction. Ex: Une couverture de survie.
2. L'emballage par au moins 2 couches d'isolation interne pour permettre d'emmagasiner de la châleur. Ex: un sac de couchage ou des couvertures.
3. La mise en place de chaufferettes sans contact direct avec la peau pour permettre un réchauffement externe sans occasionner de brûlures cutanées.
4. Une couche externe étanche à la vapeur réduit les pertes par EVAPORATION en protégeant les couches internes d'isolation de l'eau externe (pluie, neige, humidité du sol) et réduit les pertes par CONVECTION (15 % des pertes, liée au vent. Ex une couverture de survie.
5. L'isolation du sol réduit les pertes par CONDUCTION (transfert de calories par contact direct entre deux corps, 3% des pertes ). Ex: un tapis de sol.
| Tags : hypothermie
26/10/2013
Mal des montagnes: Actualisation
| Tags : montagne
26/02/2013
Combat en altitude: Le point de vue OTAN
02/07/2012
Altitude acclimatization and illness management
| Tags : altitude
18/04/2012
Médecine de montagne
| Tags : montagne
Manuel de survie US
Medical Aspects of Harsh Environments
17/04/2012
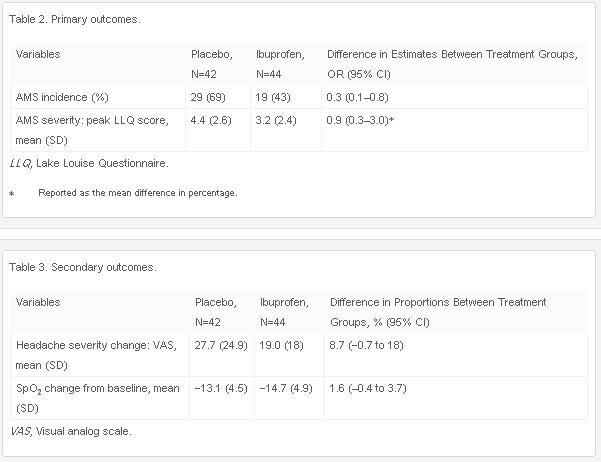
Ibuprofen pour le mal des montagnes
L'utilisation du diamox est reconnu pour la prévention du mal aigu des montagnes (Lire l'article). L'ibuprofen serait également efficace.
Ibuprofen Prevents Altitude Illness: A Randomized Controlled Trial for Prevention of Altitude Illness With Nonsteroidal Anti-inflammatories
Lipman GS et all. doi:10.1016/j.annemergmed.2012.01.019
Study objective
Acute mountain sickness occurs in more than 25% of the tens of millions of people who travel to high altitude each year. Previous studies on chemoprophylaxis with nonsteroidal anti-inflammatory drugs are limited in their ability to determine efficacy. We compare ibuprofen versus placebo in the prevention of acute mountain sickness incidence and severity on ascent from low to high altitude.
Methods
Healthy adult volunteers living at low altitude were randomized to ibuprofen 600 mg or placebo 3 times daily, starting 6 hours before ascent from 1,240 m (4,100 ft) to 3,810 m (12,570 ft) during July and August 2010 in the White Mountains of California. The main outcome measures were acute mountain sickness incidence and severity, measured by the Lake Louise Questionnaire acute mountain sickness score with a diagnosis of ≥ 3 with headache and 1 other symptom.
Results
Eighty-six participants completed the study; 44 (51%) received ibuprofen and 42 (49%) placebo. There were no differences in demographic characteristics between the 2 groups. Fewer participants in the ibuprofen group (43%) developed acute mountain sickness compared with those receiving placebo (69%) (odds ratio 0.3, 95% confidence interval 0.1 to 0.8; number needed to treat 3.9, 95% confidence interval 2 to 33). The acute mountain sickness severity was higher in the placebo group (4.4 [SD 2.6]) than individuals receiving ibuprofen (3.2 [SD 2.4]) (mean difference 0.9%; 95% confidence interval 0.3% to 3.0%)
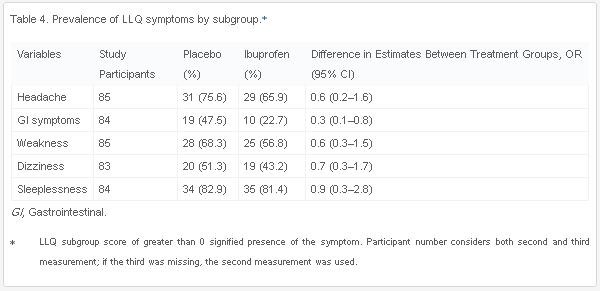
.Conclusion
Compared with placebo, ibuprofen was effective in reducing the incidence of acute mountain sickness.