20/11/2025
Chaine de survie 21ème siècle: Réflexions US
Clic sur l'image pour accéder au document
Le facteur humain reste CENTRAL
"While technology continues to transform warfare, the human element remains central to military medicine. The operational ‘kill chain’ may be accelerated by drones and artificial intelligence. However, the medical ‘survival chain’ still demands human judgement, compassion, and moral courage"
01/10/2025
Combats actuels, le mieux: Une structure chirurgicale à 1 heure
Modeling Musculoskeletal Combat Casualty Care: NATO Trauma System Performance in Large Scale Combat Operations
Cote MP et Al. JB JS Open Access. 2025 Sep 11;10(3):e25.00194. doi: 10.2106/JBJS.OA.25.00194.
Background:
It is unclear whether the current North Atlantic Treaty Organization (NATO) trauma system will be effective in the setting of Large-Scale Combat Operations (LSCO). We sought to model the efficacy of the NATO trauma system in the setting of LSCO. We also intended to model novel scenarios that could better adapt the current system to LSCO.
Methods:
We developed a discrete-event simulation model for patients with combat musculoskeletal injuries treated within the standard NATO system. The primary outcome of the model was survival. The model's health states were characterized as stable, hypovolemia, sepsis, shock, or death. The model simulated combat intensity by increasing the number of casualties up to 192 casualties per 24 hours. We explored how an augmented system (FC) and Field Hospital (FH) moved closer to the battlefront would change performance.
Results:
Mortality rates rose precipitously from a 10% baseline to 61% at 12 casualties per 24 hours in the base model. This performance was not significantly different from that of the FC model at any casualty rate. Successful evacuation of casualties was significantly more for the FH model versus the base model at 12 casualties/24 hours (47.5% vs. 39%; p = 0.046), 48 casualties/24 hours (45.5% vs. 33%; p = 0.008), and 192 casualties/24 hours (25% vs. 15.5%; p = 0.02).
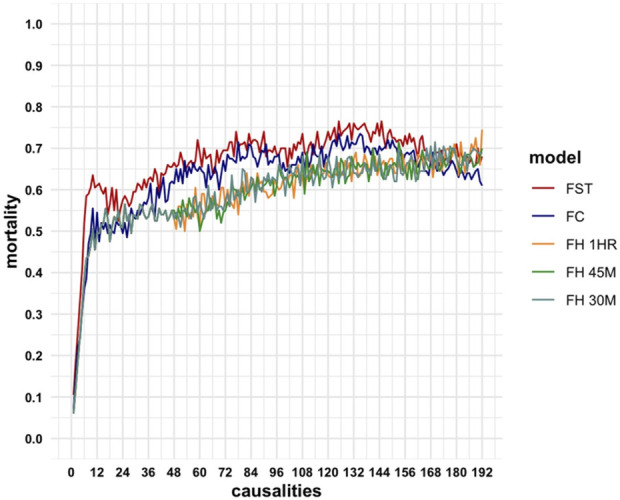
Conclusions:
The current NATO model experiences high rates of mortality in LSCO. The most effective modification entails situating Field Hospitals within one-hour of ground transport from the battlefront.
22/09/2024
Drones et Medevac: Cela avance
On connaissait le MALOY T400 mis en avant par la Royal Navy, voici ce que proposent les allemands:
mis e
Drone Grille de la société AVILUS
Quant aux Ukrainiens :

| Tags : dr
13/09/2023
Drône et évacuation: Effectif en Ukraine
Le quotidien The Economist rapporte dans un article sur ce que la médecine de guerre apprend en terres ukrainiennes, les armées de Kiev utiliseraient de gros drones cargo pour évacuer certains de ses blessés du front.
Comme l'explique le site War on the Rocks, des drones ont été utilisés dès le début de la guerre pour ravitailler troupes et blessés en matériel de soins ou en rations basiques, notamment les combattants retranchés dans l'usine Azovstal à Marioupol.
De son côté, CBC rapportait dès mars 2022 qu'une firme canadienne nommée Draganfly fournissait à Kiev de gros drones-cargos pour des missions similaires de livraison.
Le drone utilisé pourrait être un des drone de la société Malloy déjà testé par les Royal marines, probablement un T400.
| Tags : drone
12/11/2022
Triage: Encore + d'expertise à l'avant
JTS Analyzes Search and Rescue After Action Reports to Uncover Deficiencies,
Develops Performance Improvement Metrics
https://prolongedfieldcare.org/2022/03/18/joint-trauma-system-newsletter-update/
The JTS PI and CTS Operations branches published in-depth review of after action reports (AARs) from over 252 search and rescue (SAR) missions from 2018 - 2021. The report is in response to the U.S. Navy SAR’s request that JTS assess its operations. It analyzes the context in which Naval SAR operations oc- curred as well as medical procedures and patient demographics. JTS identified deficiencies in equipment, personnel, and documentation and developed a list of PI metrics. The need for standardization is keenly felt in the field. AAR comments reinforce the need for standardized equipment like cardiac kits, medication kits, and advanced life support tools. For example, SAR crews report they do not have the equipment or skills to perform rapid intubation of patients. The report was unable to conclude whether or not standardized medication kits are available to SAR teams. The report did find skills of attendant medical personal vary considerably across SAR missions. Thirty-one percent of missions were executed by a single EMT-B, while 19% were executed by a single EMP-P, and 17% were executed by two medical attendants. In some cases, both a registered nurse and physician were present, while other times only one was pre- sent.
JTS identified opportunities for improving documentation. Vague or incomplete information in the after action reports makes it more difficult to conduct accurate assessments. Accurate information is critical for mission success. Casualty classification was one area of deficiency. The report found that there is only an 81% overall accuracy in the SAR Rescuer Skill Type
casualty classification. This puts casualty classification high on the list of performance improvement (PI) priorities. Casualty classification includes all the critical information of the patient, most notably the type and severity of injury and location of the patient. It is imperative that patients are accurately classified at the start of the mission, since this determines everything from prioritizing patient care to the medical and logistical resources. A key metric for success is the comparison between the dispatched category and the assessed category of the casualty. Dispatch’s casualty classification should match the classification assessed upon the arrival at the mission destination. Having accurate information upfront is critical for SAR teams to accurately triage the casualty in advance, which dictates urgency, timing, equipment, and all other areas of mission prep. Inconsistent SAR documentation impacts the ability for SAR teams to record accurate information. For example, the DA4700 form has a list of specific mechanisms of injury (MOI), which are tailored towards battlefield en route care and not necessarily applicable to SAR operations. JTS reported roughly one fifth (55 out of 252 cases) of SAR cases recorded the MOI as either “other” or left blank. “Other” or left unchecked ultimately makes the data less useful and harder to interpret. In cases of hypothermia, the patient’s temperature was only recorded in 13% of cases. An emphasis on documentation training may
fill the gaps in SAR documentation.
The situation is further complicated by the fragmented nature of the available guidance for SAR teams. JTS discovered SAR teams rely on guidelines from multiple sources, bringing into question source credibility and guidance consistency.
The lack of training is at the root of the deficiencies. Additionally, actual mission engagements do not provide for redundancy which would lead to proficiency, proving that personnel training is of paramount importance. For instance, in one exercise, Special Operations assets had to be utilized for Casualty Evacuation (CASEVAC) purposes because the CASEVAC plan proved insufficient during the course of the exercise. The AARs recommended regular testing and evaluation of CASEVAC plans.
Response to the JTS SAR report has been positive and supportive. LCDR Paul Roszko, Director of Emergency Medical Services, Navy Medical Forces, called the report “excellent” and viewed the findings as an opportunity to improve trauma training across the Services. The report prompted Rosko to question why there is not standardized casualty cards or simulations. He would like to take real-life cases and turn them into vignettes or simulations for squadron training. JTS does include an example of a SAR casualty vignette as a tool to improve SAR training. “The data is clear that the SAR community does a lot more than just treat trauma patients,” said Rozko. “Perhaps identifying a few common medical cases or other types of commonly encountered injuries and specifying what our "standard of care" reference point is would allow the JTS PI team to provide more feedback on the quality of care provided.”
23/10/2022
Drone: Pour quoi faire ?
SOFINS 2019: A quoi pourrait servir un drone pour le soutien médical du combattant ?

Clic sur l'image pour accéder au document
| Tags : drone
12/08/2019
Soutien médical:Les enjeux du transport

Clic sur l'image pour accéder au document
Soutien médical:Les enjeux du transport
Clic sur l'image pour accéder au document
07/06/2019
Drone et SAR. C'est pour demain
The potential use of unmanned aircraft systems (drones) in mountain search and rescue operations.
----------------------------------------
Gagner du temps dans la localisation des victimes, c'est ce que pourrait apporter l'utilisation de drone. L'application opérationnelle pour la prise en charge de blessés de guerre comporte des contraintes différentes mais à n'en pas douter le train est en marche.
----------------------------------------
Objective: This study explores the potential use of drones in searching for and locating victims and of motorized transportation of search and rescue providers in a mountain environment using a simulation model.
Methods: This prospective randomized simulation study was performed in order to compare two different search and rescue techniques in searching for an unconscious victim on snow-covered ground. In the control arm, the Classical Line Search Technique (CLT) was used, in which the search is performed on foot and the victim is reached on foot. In the intervention arm, the Drone-snowmobile Technique (DST) was used, the search being performed by drone and the victim reached by snowmobile. The primary outcome of the study was the comparison of the two search and rescue techniques in terms of first human contact time.
Results: Twenty search and rescue operations were conducted in this study. Median time to arrival at the mannequin was 57.3 min for CLT, compared to 8.9 min for DST. The median value of the total searched area was 88,322.0 m2 for CLT and 228,613.0 m2 for DST. The median area searched per minute was 1489.6 m2 for CLT and 32,979.9 m2 for DST (p b 0.01 for all comparisons).
| Operation | Recherche classique | Recherche par drone | ||||
|---|---|---|---|---|---|---|
| First human contact (min) |
Total searched area (m 2 ) |
Searched area for a minute (m 2 /min) |
First human contact (min) |
Total searched area (m 2 ) |
Searched area for a minute (m 2 /min) |
|
| 1 | 39.0 | 66,408 | 1702.8 | 7.7 | 168,395 | 28,065.8 |
| 2 | 53.1 | 78,209 | 1475.6 | 8.2 | 217,624 | 33,225.1 |
| 3 | 67.1 | 88,664 | 1323.3 | 8.5 | 239,602 | 35,080.8 |
| 4 | 95.0 | 120,891 | 1272.5 | 11.2 | 310,981 | 32,734.8 |
| 5 | 50.2 | 85,861 | 1717.2 | 5.6 | 192,224 | 49,162.1 |
| 6 | 95.2 | 104,479 | 1099.8 | 13.1 | 346,268 | 30,294.7 |
| 7 | 54.0 | 98,385 | 1821.9 | 7.4 | 144,480 | 25,302.9 |
| 8 | 61.1 | 77,378 | 1268.5 | 4.2 | 138,945 | 54,488.2 |
| 9 | 59.1 | 87,980 | 1503.7 | 9.7 | 266,722 | 33,340.3 |
| 10 | 56.1 | 99,375 | 1774.6 | 12.9 | 313,525 | 27,968.3 |
| Median (25–75%) |
57.3 a (52.3–74.0) |
88,322.0 b (78,001.3–100,651.0) |
1489.7 c (1271.5–1731.6) |
8.4 a (6.9–11.6) |
228,613.0 b (162,416.0–311,617.0) |
32,979.9 c (28,041.4–8601.1) |
Conclusions: In conclusion, a wider area can be searched faster by drone using DST compared to the classical technique, and the victim can be located faster and reached earlier with rescuers transported by snowmobile
| Tags : drone
31/05/2019
Hémorragie du tronc non compressible: MEDEVAC COURTE
Impact of prehospital medical evacuation (MEDEVAC) transport time on combat mortality in patients with non-compressible torso injury and traumatic amputations: a retrospective study
BACKGROUND:
In combat operations, patients with traumatic injuries require expeditious evacuation to improve survival. Studies have shown that long transport times are associated with increased morbidity and mortality. Limited data exist on the influence of transport time on patient outcomes with specific injury types. The objective of this study was to determine the impact of the duration of time from the initial request for medical evacuation to arrival at a medical treatment facility on morbidity and mortality in casualties with traumatic extremity amputation and non-compressible torso injury (NCTI).
METHODS:
We completed a retrospective review of MEDEVAC patient care records for United States military personnel who sustained traumatic amputations and NCTI during Operation Enduring Freedom between January 2011 and March 2014. We grouped patients as traumatic amputation and NCTI (AMP+NCTI), traumatic amputation only (AMP), and neither AMP nor NCTI (Non-AMP/NCTI). Analysis was performed using chi-squared tests, Fisher's exact tests, Cochran-Armitage Trend tests, Shapiro-Wilks tests, Wilcoxon and Kruskal-Wallis techniques and Cox proportional hazards regression modeling.
RESULTS:
We reviewed 1267 records, of which 669 had an injury severity score (ISS) of 10 or greater and were included in the analysis. In the study population, 15.5% sustained only amputation injuries (n=104, AMP only), 10.8% sustained amputation and NCTI (n=72, AMP+NCTI), and 73.7% did not sustain either an amputation or an NCTI (n=493, Non-AMP/NCTI). AMP+NCTI had the highest mortality (16.7%) with transport time greater than 60 min. While the
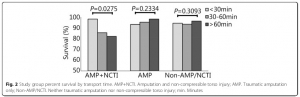
AMP+NCTI group had decreasing survival with longer transport times, AMP and Non-AMP/NCTI did not exhibit the same trend.
CONCLUSIONS:
A decreased transport time from the point of injury to a medical treatment facility was associated with decreased mortality in patients who suffered a combination of amputation injury and NCTI. No significant association between transport time and outcomes was found in patients who did not sustain NCTI. Priority for rapid evacuation of combat casualties should be given to those with NCTI.
08/04/2019
CCATT: LA voie à suivre pour les EVAC
En Route Resuscitation – Utilization of CCATT to Transport and Stabilize Critically Injured and Unstable Casualties
Maddry JK et Al Mil Med. 2018 Dec 7. doi: 10.1093/milmed/usy371.
--------------------------------------
Une démarche qui prône l'emploi de spécialistes ayant une pratique régulière et avancée de la réanimation et de l'anesthésie du traumatisé pour le transport des blessés de guerre. Elle doit être rapprochée du concept des MERT-Enhanced UK.
--------------------------------------
Introduction:
The U.S. Air Force utilizes specialized Critical Care Air Transport Teams (CCATT) for transporting “stabilized” patients. Given the drawdown of military forces from various areas of operation, recent
CCATT operations have increasingly involved the evacuation of unstable and incompletely resuscitated patients from far forward, austere locations. This brief report describes unique cases representative of the evolving CCATT mission and provides future direction for changes in doctrine and educational requirements in preparation for en route combat casualty care. Methods and Materials: This case series describes three patients who required significant resuscitation during CCATT transport from austere locations between April and November 2017. Approval for this project was received from the US Air Force 59th Medical Wing Institutional Review Board as non-research.
Results:
Case 1:
CCATT was dispatched to transport patient 1 who was reported to have a head injury after a fall. Upon evaluation of the patient onboard the aircraft, it was discovered that the patient was in cardiac arrest. Cardiopulmonary resuscitation was performed during tactical takeoff with frequent combat maneuvers. The patient developed a palpable pulse after three rounds of CPR, three doses of epinephrine, and one unit of packed red blood cells. Point of care laboratory analysis demonstrated a profoundly elevated lactate level. Cyanide poisoning was a concern but there was no antidote available in the available equipment set. After delivery to a medical facility, blood samples were positive for cyanide. Over the next 2 weeks, the patient improved and was discharged home, neurologically intact.
Case 2:
Patient 2 sustained complex blast injuries and bilateral lower extremity amputations. He required early transport for continuous renal replacement therapy (CRRT). The patient received 200 units of blood products in the 24 hours prior to transport and developed renal failure, pulmonary edema, and elevated ICP. During the 7 hour flight, Patient 2 received frequent adjustments of vasopressor medications, multiple Dakins solution soaks and flushes, and 1 unit of fresh frozen plasma. He mained alive 2 months later.
Case 3:
The team was notified to collect an urgent patient with a blast lung injury and bilateral lower extremity amputations. The ground team encountered difficulty ventilating the patient. Patient 3 arrived in the back of a pickup truck accompanied by medics and being bag valve mask ventilated with a pulse oximetry reading of 65%. He was secured to the floor of the aircraft which departed within 5 minutes of arrival. An ultrasound of the lungs showed no pneumothorax. By the end of the flight, the patient’s oxygen saturation had risen to 95% and he was delivered to the emergency department in stable condition. He later passed away in the operating room due to severe blast lung and cardiac contusion.
Conclusion: This brief report demonstrates the need of CCATT in the transport of unstable patients from forward deployed locations. The Air Force has adapted and is continuing to adapt CCATT training, equipment, onboard diagnostics and therapies, and team members’ clinical skills to meet en route care combat casualty needs.
16/03/2019
CASE EVAC/MEDEVAC: Besoin de clarification
A Descriptive Analysis of Causalities Undergoing CASEVAC from the Point-of-Injury in the Department of Defense Trauma Registry
The recent conflicts in Iraq and Afghanistan entail an asymmetric battlefield without clearly defined forward lines of troops as seen in previous wars. Accordingly, the United States military medical services have increasingly adopted casualty evacuation (CASEVAC) platforms. We describe CASEVAC events reported within the Department of Defense Trauma Registry (DODTR).
This is a secondary analysis of previously published data from two datasets spanning from 2007 through 2017. We isolated casualties within our dataset that had a documented evacuation method from the point-of-injury other than dedicated medical evacuation platforms (e.g., MEDEVAC, etc.).
During OPERATION IRAQI FREEDOM, three casualties underwent CASEVAC. The median age was 30 and all were male. Most sustained injuries from explosives (67%) and the median composite injury scores were low (10). The most frequent seriously injured body region was the thorax (67%). All survived to hospital discharge. During operations in Afghanistan (OPERATION ENDURING FREEDOM, OPERATION FREEDOMS SENTINEL, OPERATION NEW DAWN), 248 casualties underwent CASEVAC. The median age was 28 and most (96%) were male. Most sustained injuries from explosives (58%) and the median injury score was low (9). The most frequent seriously injured body region was the extremities (24%). Most (97%) survived to hospital discharge. During OPERATION INHERENT RESOLVE, 247 casualties underwent CASEVAC. The median age was 21 and most (96%) were male. The majority sustained injuries from explosives (61%) and the median injury score was low (9). The most frequent seriously injury body region was the extremities (27%). Most survived to hospital discharge (94%).
In our dataset, CASEVAC events most frequently involved US military personnel service members with most surviving to hospital discharge. Developing new terminology that distinguishes different types of CASEVAC would allow for more accurate future analyses of casualty evacuation and outcomes – such as those transports that are truly in a non-medical versus the various medical platforms that do not fall with into the confines of the MEDEVAC platforms.
02/11/2018
Blessés admis en role 2: Le bilan afghan
A Review of Casualties Transported to Role 2 Medical Treatment Facilities in Afghanistan.
---------------------------------------
Ce document met en évidence tout l'apport d'une chaine coordonnée de prise en charge du traumatisé par des équipes entraînées appliquant une stratégie médico-chirurgicale moderne.
---------------------------------------
Critically injured trauma patients benefit from timely transport and care. Accordingly, the provision of rapid transport and effective treatment capabilities in appropriately close proximity to the point of injury will optimize time and survival. Pre-transport tactical combat casualty care, rapid transport with en route casualty care, and advanced damage control resuscitation and surgery delivered early by small, mobile, forward-positioned Role 2 medical treatment facilities have potential to reduce morbidity and mortality from trauma. This retrospective review and descriptive analysis of trauma patients transported from Role 1 entities to Role 2 facilities in Afghanistan from 2008 to 2014 found casualties to be diverse in affiliation and delivered by various types and modes of transport. Air medical evacuation provided transport for most patients, while the shortest transport time was seen with air casualty evacuation. Although relatively little data were collected for air casualty evacuation, this rapid mode of transport remains an operationally important method of transport on the battlefield. For prehospital care provided before and during transport, continued leadership and training emphasis should be placed on the administration and documentation of tactical combat casualty care as delivered by both medical and non-medical first responders.
08/09/2018
Le TCCC dans la vraie vie
Survey of Casualty Evacuation Missions Conducted by the 160th Special Operations Aviation Regiment During the Afghanistan Conflict.
BACKGROUND:
Historically, documentation of prehospital combat casualty care has been relatively nonexistent. Without documentation, performance improvement of prehospital care and evacuation through data collection, consolidation, and scientific analyses cannot be adequately accomplished. During recent conflicts, prehospital documentation has received increased attention for point-of-injury care as well as for care provided en route on medical evacuation platforms. However, documentation on casualty evacuation (CASEVAC) platforms is still lacking. Thus, a CASEVAC dataset was developed and maintained by the 160th Special Operations Aviation Regiment (SOAR), a nonmedical, rotary-wing aviation unit, to evaluate and review CASEVAC missions conducted by their organization.
METHODS:
A retrospective review and descriptive analysis were performed on data from all documented CASEVAC missions conducted in Afghanistan by the 160th SOAR from January 2008 to May 2015. Documentation of care was originally performed in a narrative after-action review (AAR) format. Unclassified, nonpersonally identifiable data were extracted and transferred from these AARs into a database for detailed analysis. Data points included demographics, flight time, provider number and type, injury and outcome details, and medical interventions provided by ground forces and CASEVAC personnel.
RESULTS:
There were 227 patients transported during 129 CASEVAC missions conducted by the 160th SOAR. Three patients had unavailable data, four had unknown injuries or illnesses, and eight were military working dogs. Remaining were 207 trauma casualties (96%) and five medical patients (2%). The mean and median times of flight from the injury scene to hospital arrival were less than 20 minutes. Of trauma casualties, most were male US and coalition forces (n = 178; 86%). From this population, injuries to the extremities (n = 139; 67%) were seen most commonly. The primary mechanisms of injury were gunshot wound (n = 89; 43%) and blast injury (n = 82; 40%). The survival rate was 85% (n = 176) for those who incurred trauma. Of those who did not survive, most died before reaching surgical care (26 of 31; 84%).
CONCLUSION:
Performance improvement efforts directed toward prehospital combat casualty care can ameliorate survival on the battlefield. Because documentation of care is essential for conducting performance improvement, medical and nonmedical units must dedicate time and efforts accordingly. Capturing and analyzing data from combat missions can help refine tactics, techniques, and procedures and more accurately define wartime personnel, training, and equipment requirements. This study is an example of how performance improvement can be initiated by a nonmedical unit conducting CASEVAC missions.
08/08/2018
A 400M allemand : Prêt pour les MEDEVAC

L'Allemagne dispose à présent de la capacité d'évacuation aéromédicale à bord d'un A400M. Le premier kit « Intensive care aeromedical evacuation » (ICAE) a été mis en service ce 1er août, avec un délai d'alerte à 12 heures. Au total, la Luftwaffe disposera à terme de quatre kits, intégrable aux A400M en quatre heures, pour prendre en charge le rapatriement de blessés - aussi bien allemands qu'européens, voire des autres pays membres de l'OTAN.
Le kit ICAE permettra de prendre en charge jusqu'à six blessés allongés avec oxygénothérapie et appareils de réanimation, dont deux en unité de soins intensifs, deux blessés de catégorie intermédiaire et deux blessés plus légers. L'équipe médicale est quant à elle composée de 11 personnels, de différentes spécialités. (source).
12/04/2018
La vitesse ne fait pas tout
Speed is not everything: Identifying patients who may benefit from helicopter transport despite faster ground transport.
------------
Ne pas perdre de temps est bien. Mais il ne faut pas oublier également que la réalisation de gestes avancés de réanimation est aussi utile en préhospitalier. Ceci milite pour la constitution d'équipes dont l'expertise en matière de gestion des voies aériennes/Trauma thoracique-Crânien est le métier. Cette question se pose tout particulièrement pour les vecteurs d'EVASAN à voilure tournante.
------------
BACKGROUND:
Helicopter emergency medical services (HEMS) have demonstrated survival benefits over ground emergency medical services (GEMS) for trauma patient transport. While HEMS speed is often-cited, factors such as provider experience and level of care may also play a role. Our objective was to identify patient groups that may benefit from HEMS even when prehospital time for helicopter utilization is longer than GEMS transport.
METHODS:
Adult patients transported by HEMS or GEMS from the scene of injury in the Pennsylvania State Trauma Registry were included. Propensity score matching was used to match HEMS and GEMS patients for likelihood of HEMS, keeping only pairs in which the HEMS patient had longer total prehospital time than the matched GEMS patient. Mixed-effects logistic regression evaluated the effect of transport mode on survival while controlling for demographics, admission physiology, transfusions, and procedures. Interaction testing between transport mode and existing trauma triage criteria was conducted and models stratified across significant interactions to determine which criteria identify patients with a significant survival benefit when transported by HEMS even when slower than GEMS.
RESULTS:
From 153,729 eligible patients, 8,307 pairs were matched. Helicopter emergency medical services total prehospital time was a median of 13 minutes (interquartile range, 6-22) longer than GEMS. Patients with abnormal respiratory rate (odds ratio [OR], 2.39; 95% confidence interval [CI], 1.26-4.55; p = 0.01), Glasgow Coma Scale score of 8 or less (OR, 1.61; 95% CI, 1.16-2.22; p < 0.01), and hemo/pneumothorax (OR, 2.25; 95% CI, 1.06-4.78; p = 0.03) had a significant survival advantage when transported by HEMS even with longer prehospital time than GEMS. Conversely, there was no association between transport mode and survival in patients without these factors (p > 0.05).
CONCLUSION:
Patients with abnormal respiratory rate, Glasgow Coma Scale score of 8 or less, and hemo/pneumothorax benefit from HEMS transport even when GEMS transport was faster. This may indicate that these patients benefit primarily from HEMS care, such as advanced airway and chest trauma management, rather than simply faster transport to a trauma center.
| Tags : evasan
18/10/2017
On peut rêver

Philippe Chapleau nous apprend que dans le cadre de son déploiement en Europe, les 1900 soldats de la 1st Air Cavalry Brigade disposera disposeront de 12 Chinook, 38 Black Hawk, 24 Apache et 15 Black Hawk médicalisés. On peut rêver.
| Tags : medevac
26/03/2017
MEDEVAC Sangaris: Du médical avant tout
Évacuations médicales aériennes tactiques et stratégiques en République centrafricaine au cours de l’opération « Sangaris ». Synthèse des onze premiers mois d’opérations
Beylot V. et Al. médecine et armées, 2016, 44, 4, 087-096
-------------------------------------
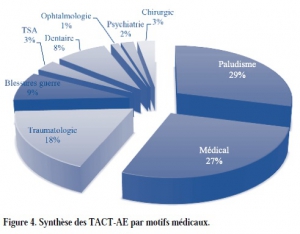
Un état des lieux intéressants qui n'est pas sans rappeler l'histoire de nos anciens confrontés à l'isolement et à la dureté du climat. Les causes médicales de MEDEVAC en première ligne dont le Paludisme ?, les envenimations scorpioniques, les problèmes dentaires. Les blessures par armes de guerre apparaissent beaucoup moins fréquentes. Le contexte d'intervention: une guerre civile, les élongations et les problèmes climatiques expliquent beaucoup de chose. Une grosse différence l'emploi quasi systématique, hors Bangui, du vecteur aérien pour les medevac, vecteur ldont la mise en oeuvre a pu être optimisé par un centre de coordination dont le rôle est essentiel.
-------------------------------------
Au cours des onze premiers mois de l’opération « Sangaris », 249 évacuations médicales aériennes tactiques et 186 évacuations médicales aériennes stratégiques ont été réalisées. Nous proposons ici une présentation synthétique de ces évacuations. Dans les motifs d’évacuation, la place importante du paludisme (29 % des évacuations tactiques) est un reflet de l’épidémie à laquelle les forces françaises ont été confrontées. Les conditions de déploiement en interposition ont pu amplifier l’impact psychiatrique de cette mission (28 % des évacuations stratégiques) et participer à la réouverture du sas de fin de mission. La place des blessures de guerres (9 % des évacuations tactiques et 13 % des évacuations stratégiques) majoritairement dues à des éclats de grenades reste importante et illustre le risque inhérent à cet engagement.
Enfin, si la chaîne de santé complète déployée au plus proche, en passant notamment par la nomadisation des équipes héliportées, a permis d’assurer un soutien médical de qualité, l’étendue de ce théâtre nous interpelle sur les délais et la catégorisation utilisée lors des évacuations tactiques.
| Tags : medevac
17/03/2017
CSAR: Expérience israélienne
Prehospital Blood Transfusion During Aeromedical Evacuation of Trauma Patients in Israel: The IDF CSAR Experience.
Chen J et Al. Mil Med. 2017 Mar;182(S1):47-52
---------------------------------
L'expérience d'une unité CSAR un peut particulière, très entraînée et dépendant des Forces spéciales. La transfusion se fait sur la basse d'un njugement clinique. Il est intéressant de voir que ces équipes intubent, drainent, exsuffle autant qu'elles posent de garrots.
---------------------------------
BACKGROUND: Data regarding the effect of prehospital blood administration to trauma patients during short-to-moderate time evacuations is scarce. The Israel Air Force Airborne Combat Search and Rescue is the only organization that deals with aeromedical evacuation for both military and civilian casualties in Israel and the only one with the ability to give blood in the prehospital setting.
METHODS: Data on packed red blood cells (PRBCs) administration in the evacuation missions from January 2003 to June 2010 were analyzed and actual transfusion practice was compared to clinical practice guidelines (CPGs).
RESULTS: Over the studied 101 months, a total of 1,721 patients were evacuated by Combat Search and Rescue. Of these, 87 (5.1%) trauma patients were transfused with PRBC. Demographics included 83% male and 17% female with a median age of 23 years. Main mechanisms of injury included gunshot wounds (36%), motor vehicle accidents (28%), and blast injuries (24%) with an average of 2.6 injured regions per casualty. The most commonly injured body regions included lower extremities (52%), chest (45%), and abdomen (38%). Overall, 10 (11%) casualties died. Lifesaving intervention included tourniquets (27%), endotracheal intubation (24%), tube thoracostomy (24%), and needle thoracostomy (21%) times. For 98% of the patients, clinical judgment led to administration of red blood cells before indicated by the CPG. The heart rate tended to decrease during the evacuation, whereas there was no clear trend in systolic or diastolic blood pressure or shock index.
CONCLUSIONS: In our aeromedical experience, transfusion of PRBCs for trauma patients was safe, feasible, and most likely beneficial. PRBCs were administered according to the flight surgeons' clinical judgment and not in complete adherence to CPGs in most cases. Data collected from this and similar studies worldwide have led to change in CPGs with the shift from hypertensive resuscitation to hypotensive-hemostatic Remote Damage Control Resuscitation.
18/01/2017
MEDEVAC de la BSS: En gros que fait on ?
Forward medevac during Serval and Barkhane operations in Sahel: A registry study.
Carfantan C, et Al. Injury. 2017 Jan;48(1):58-63.
-----------------------------------
Une activité particulièrement sensible dont la lecture permet de comprendre toute la complexité de la prise en charge de nos soldats dans un contexte d'élongation majeure. On comprend également tous les enjeux de positionnement d'équipes sanitaires ayant la maîtrise de certaines pratiques avancées de réanimation préhospitalière.
-----------------------------------
INTRODUCTION:
The French army has been deployed in Mali since January 2013 with the Serval Operation and since July 2014 in the Sahel-Saharan Strip (SSS) with the Barkhane Operation where the distances (up to 1100km) can be very long. French Military Medical Service deploys an inclusive chain from the point of injury (POI) to hospital in France. A patient evacuation coordination cell (PECC) has been deployed since February 2013 to organise forward medical evacuation (MEDEVAC) in the area between the POI and three forward surgical units. The purpose of this work was to study the medical evacuation length and duration between the call for Medevac location accidents and forward surgical units (role 2) throughout the five million square kilometers French joint operation area.
MATERIALS AND METHODS:
Our retrospective study concerns the French patients evacuated by MEDEVAC from February 2013 to July 2016. The PECC register was analysed for patients' characteristics, NATO categorisation of gravity (Alpha, Bravo or Charlie who must be respectively at hospital facility within 90min, 4h or 24h), medical motive for MEDEVAC and the time line of each MEDEVAC (from operational commander request to entrance in role 2).
RESULTS:
A total of 1273 French military were evacuated from February to 2013 to July 2016; 533 forward MEDEVAC were analysed. 12,4% were Alpha, 28,1% Bravo, 59,5% Charlie. War-related injury represented 18,2% of MEDEVAC. The median time for Alpha category MEDEVAC patients was 145min [100-251], for Bravo category patients 205min [125-273] and 310min [156-669] for Charlie. The median distance from the point of injury to role 2 was 126km [90-285] for Alpha patients, 290km [120-455] km for Bravo and 290km [105-455] for Charlie.
CONCLUSIONS:
Patient evacuation in such a large area is a logistic and human challenge. Despite this, Bravo and Charlie patients were evacuated in NATO recommended time frame. However, due to distance, Alpha patients time frame was longer than this recommended by NATO organisation. That's where French doctrine with forward medical teams embedded in the platoons is relevant to mitigate this distance and time frame challenge.
| Tags : evasan