30/11/2025
Reco Sauvetage en montagne ICAR

Garrot et grand froid: Possible ? ET bien OUI
Tourniquet self-application assessment in cold
weather conditions
Benítez YC et al. BMC Emergency Medicine (2023) 23:101
----------------------------
Le chox d'un garrot tactique n'est pas simple. Le CAT et le SOF-T sont parmi les plus répanduS. LE CoTCCC a évalué ses tourniquets et fait quelques propositions (1). Ces dernières ne prennet pas en compte certains besoins spécifiques comme leur emploi en zone grand froid ou en milieu maritime salin. C'est ce que propose de faire ce travail. Deux remarques: le SOFT-T ne fait pas partie des dispositifs testés. Le garrot OMNA semble être celui dont l'emploi est le plus facile dans ce contexte. Il ne s'agit pas d'un tourniquet mais d'un garrot à crématillère.
----------------------------
Background
Our study aimed to assess the ability of nonmedical civilians to self-apply extremity tourniquets in coldv weather conditions while wearing insulating technical clothing after receiving basic training.
Methods
A field study was conducted among 37 voluntary participants of an expedition party to the Spanish Antarctic base. The researchers assessed the participant’s ability to self-apply five commercial extremity tourniquets (CAT, OMNA, RMT, SWAT-T, and RATS) over cold-weather clothing and their achieved effectiveness for vascular occlusion. Upper extremity self-application was performed with a single-handed technique (OHT), and lower extremity applying a two-handed technique (THT). Perceptions of self-application ease mean values±standard
deviation (SD) were compared by applying a 5% statistical significance threshold. Frequency count determined tourniquet preference.
Results
All the tested ETs, except the SWAT-T, were properly self-applied with an OHT, resulting in effective vascular occlusion in the upper extremity. The five devices tested were self-applied correctly in the lower extremities using THT.
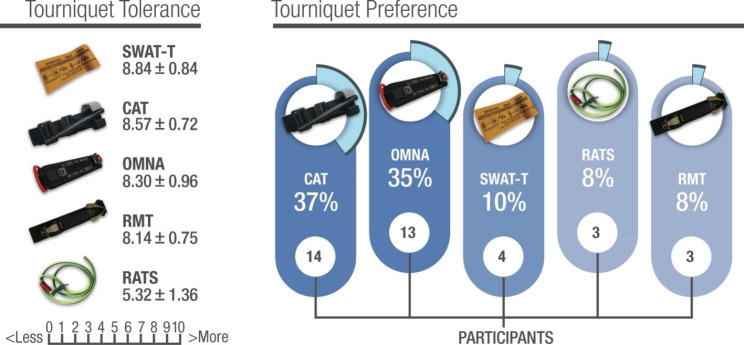
The ratcheting marine-designed OMNA ranked the highest for application easiness on both the upper and lower extremities, and the windlass CAT model was the preferred device by most participants.
Conclusions
Civilian extremity tourniquet self-application on both upper and lower extremities can be
accomplished in cold weather conditions despite using cold-weather gloves and technical clothing after receiving brief training. The ratcheting marine-designed OMNA ranked the highest for application ease, and the windlass CAT model was the preferred device
Triage et lill zone en ukraine.
Deux intérêts: Les nouvelles modalités de triage liées aux zones de déni d'accès ET l'importance de la gestion des garrots.
28/11/2025
Le MARCHE en ambiance grand froid

26/11/2025
Réchauffement cutané acif: Attention
Methods:
each test.
Results:

Conclusions:
21/11/2025
DAS 2025:Çeco Intubation difficile imprévue
Difficult Airway Society 2025 guidelines for management of unanticipated difficult tracheal intubation in adults
![]()
Hypothermie: Plutôt un blessé au sec dès que possible que mouillé
Effect of wet clothing removal on skin temperature in subjects exposed to cold and wrapped in a vapor barrier: a human, randomized, crossover field study
Hagen LT et Al. BMC Emergency Medicine volume 24, Article number: 18 (2024)
----------------------
La présence de vêtements humides chez un blessé pris en charge dans un contexte tactique ne permet pas le plus souvent de remplacer ceux ci par des effets secs. Cela est tout à fait acceptable si la prévention de l'hypothermie fait appel à un emballage avec plusieurs couches dont une faisance office de barrière contre la vapeur (1). L'idéal est quand même de remplacer ceux ci au plus tôt par des effets secs car alors la prise en charge de cette hypthermie sera de bien meilleure qualité
----------------------
Background
Prehospital care for cold-stressed and hypothermic patients focuses on effective insulation and rewarming. When encountering patients wearing wet clothing, rescuers can either remove the wet clothing before isolating the patient or isolate the patient using a vapor barrier. Wet clothing removal increases skin exposure but avoids the need to heat the wet clothing during rewarming. Leaving wet clothing on will avoid skin exposure but is likely to increase heat loss during rewarming. This study aimed to evaluate the effect of wet clothing removal compared to containing the moisture using a vapor barrier on skin temperature in a prehospital setting.
Methods
This randomized crossover experimental field study was conducted in a snow cave in Hemsedal, Norway. After an initial cooling phase of 30 min while wearing wet clothes, the participants were subjected to one of two rewarming scenarios: (1) wet clothing removal and wrapping in a vapor barrier, insulating blankets, and windproof outer shell (dry group) or (2) wrapping in a vapor barrier, insulating blankets, and windproof outer shell (wet group). The mean skin temperature was the primary outcome whereas subjective scores for both thermal comfort and degree of shivering were secondary outcomes. Primary outcome data were analyzed using the analysis of covariance (ANCOVA).
Results
After an initial decrease in temperature during the exposure phase, the dry group had a higher mean skin temperature compared to the wet group after only 2 min. The skin-rewarming rate was highest in the initial rewarming stages for both groups, but increased in the dry group as compared to the wet group in the first 10 min.
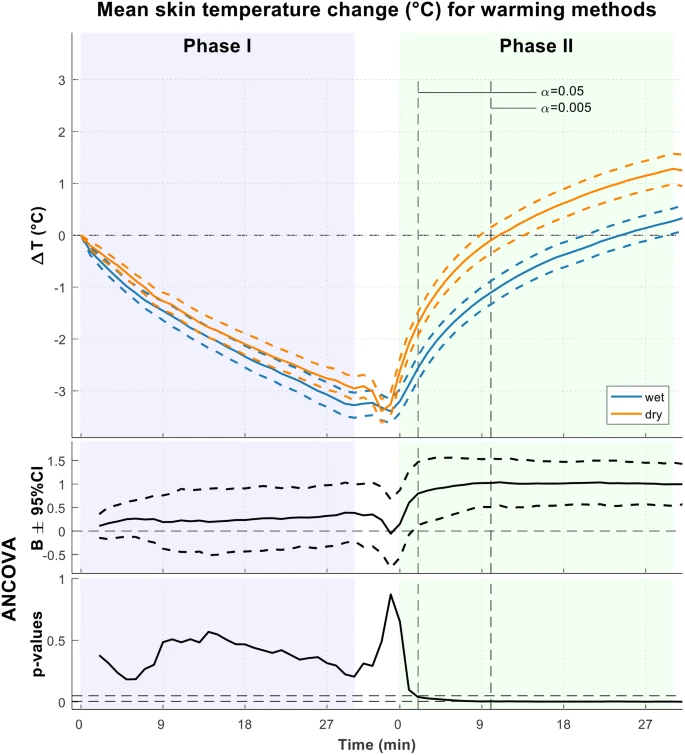
Return to baseline temperature occurred significantly faster in the dry group (mean 12.5 min [dry] vs. 28.1 min [wet]). No intergroup differences in the subjective thermal comfort or shivering were observed.
Conclusion
Removal of wet clothing in combination with a vapor barrier increases skin rewarming rate compared to encasing the wet clothing in a vapor barrier, in mild cold and environments without wind.
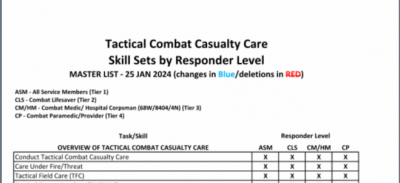
Pratiques gestuelles et niveaux de compétence chez les US
20/11/2025
Chaine de survie 21ème siècle: Réflexions US
Clic sur l'image pour accéder au document
Le facteur humain reste CENTRAL
"While technology continues to transform warfare, the human element remains central to military medicine. The operational ‘kill chain’ may be accelerated by drones and artificial intelligence. However, the medical ‘survival chain’ still demands human judgement, compassion, and moral courage"