29/10/2022
Refroidir la brulure: OUI
The effect of 20 minutes of cool running water first aid within three hours of thermal burn injury on patient outcomes: A systematic review and meta-analysis
Griffin B. et Al. Australas Emerg Care. 2022 Dec;25(4):367-376.
Background:
Burn injuries are a leading cause of morbidity that can result in devastating disability and poor quality of life for survivors. This systematic review aimed to synthesise evidence regarding the effect of 20 minutes of cool running water (CRW) within three hours of injury on outcomes of patients with thermal burn injuries.
Methods:
This systematic review was conducted in reference to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Multiple databases (PubMed, EMBASE, CENTRAL, CINAHL Complete via EBSCO, PROQUEST Dissertations and Theses), and the Australia New Zealand Clinical Trial Registry were searched for eligible studies published in English and Chinese, without date restriction. Meta-analyses were undertaken Methodological quality of studies was assessed by using Downs and Black Checklist.
Results:
Of 323 records, seven studies were included. The majority (67%) of studies were conducted in Australia and New Zealand. The methodological quality was ranked between 'fair' and 'good'. Twenty minutes of CRW within the first three hours of burn injury significantly decreased the odds of patients requiring skin grafting and surgical intervention for wound management.
Conclusions:
There is considerable evidence suggesting the application of 20 min of CRW within the first three hours of injury improves outcomes for patients with burn injury. Consensus between burn organisations and collaborative efforts to translate evidence into practice are needed to optimise burn first aid care which can improve patient outcomes globally.
African Journal of Emergency Medicine

Le Service de Santé des Armées
23/10/2022
Drone: Pour quoi faire ?
SOFINS 2019: A quoi pourrait servir un drone pour le soutien médical du combattant ?

Clic sur l'image pour accéder au document
| Tags : drone
21/10/2022
Plyo intraosseux ? Pas si simple
Intraosseous administration of freeze-dried plasma in the prehospital setting
Rittblat M et Al. Isr Med Assoc J. 2022 Sep;24(9):591-595.
Background:
Freeze dried plasma (FDP) is a commonly used replacement fluid in the prehospital setting when blood products are unavailable. It is normally administered via a peripheral intravenous (PIV) line. However, in severe casualties, when establishing a PIV is difficult, administration via intraosseous vascular access is a practical alternative, particularly under field conditions.
Objectives:
To evaluate the indications and success rate of intraosseous administration of FDP in casualties treated by the Israel Defense Forces (IDF).
Methods:
A retrospective analysis of data from the IDF-Trauma Registry was conducted. It included all casualties treated with FDP via intraosseous from 2013 to 2019 with additional data on the technical aspects of deployment collected from the caregivers of each case.
Results:
Of 7223 casualties treated during the study period, intravascular access was attempted in 1744; intraosseous in 87 of those. FDP via intraosseous was attempted in 15 (0.86% of all casualties requiring intravascular access). The complication rate was 73% (11/15 of casualties).
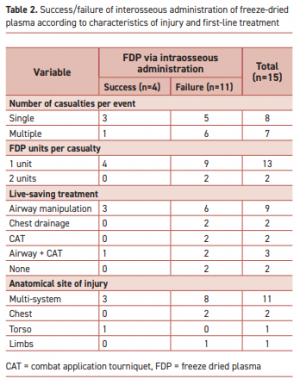
"According to the manufacturer’s specifications, the reconstituted lyophilized plasma product is delivered from a glass bottle with the rate of infusion determined primarily by gravity. This procedure precludes the care providers from applying external pressure to increase the plasma infusion rate. Therefore, the pressure gradient is determined primarily by gravity with respect to height of the bottle."
Complications were more frequent when the event included multiple casualties or when the injury included multiple organs. Of the 11 failed attempts, 5 were reported as due to slow flow of the FDP through the intraosseous apparatus. Complications in the remaining six were associated with deployment of the intraosseous device.
Conclusions:
Administration of FDP via intraosseous access in the field requires a high skill level.
| Tags : intraosseux
04/10/2022
NAEMSP Prehospital Airway Position Papers
The National Association of EMS Physicians Compendium of Airway Management Position Statements and Resource Documents
Clic sur le titre pour accéder à la page de présentation des documents
| Tags : airway
Pansement hémostatique et altitude: C'est OK
Hemostatic Effects of Bio-Zeolite Gauze and QuikClot Combat Gauze on Major Bleeding in Rabbits Acutely Exposed to High Altitude
Yi-jun J et Al. Prehosp Emerg Care. 2022 Sep 28;1-8
Objective:
Hemostatic gauze application is an effective way to control major bleeding, which is the most common cause of death in trauma in both civilian and military settings. Coagulation derangement after acute exposure to high altitude might alter the effects of hemostatic gauzes. The present study aimed to observe the hemostatic effects of bio-zeolite gauze (BZG) and QuikClot Combat Gauze® (QCG) on major bleeding in rabbits acutely exposed to high altitude.
Methods:
Sixty rabbits were randomly and evenly divided into six groups. Animal models of simulated blast- and fragment-induced inguinal major bleeding were prepared in lower altitude and high-altitude areas, and BZG, QCG, and ordinary gauze without hemostatic material were used to control bleeding. The primary outcomes included immediate hemostasis rate, blood loss, and survival rate, while the secondary outcomes included hemodynamic parameters, laboratory examinations, and coagulation-relevant markers.
Results:
The overall effects of BZG and QCG were better than those of ordinary gauze, with a higher immediate hemostatic rate, less blood loss, and higher survival rate at 90 min after gauze application and higher red blood cell and platelet counts and lower creatinine level at 30 min after gauze application in lower altitude. The concentrations of coagulation factor XII and factor X in rabbits acutely exposed to high altitude were significantly lower than those in lower altitude. At high altitude, the hemostatic effects of BZG did not decrease significantly compared to those in the lower altitude, whereas those of ordinary gauze and QCG decreased significantly at high altitude compared to those in the lower altitude.
Conclusions:
Coagulation derangement after acute exposure to high altitude has negative effects on ordinary gauze and QCG but has no significant negative hemostatic effects on BZG.