22/05/2011
Perfusion et oxygénation tissulaire
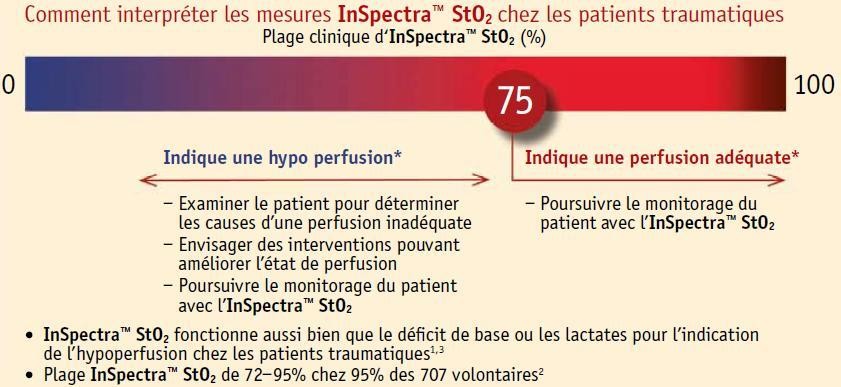
Un des enjeux de la prise en charge du blessé de guerre est le maintien d'une perfusion issulaire adaptée. Malheureusement la détection de cette dernière est difficile.
Un des outils est la mesure de l'oxygénation tissulaire (la StO2). Le document lié ici qui fait la synthèse des avancées importantes en matière de prise en charge du blessé de guerre aborde ce sujet en pages 266-267.
http://www.ecomed-services.com/downloads/Inspectra%20St02...

Des dispositifs portables sont maintenant disponibles. C'est le cas de l' InSpectraTM StO2 Spot Check.
Pour en savoir plus ici.
Quelques explications ici.
Ce type d'équipement paraît particulièrement intéressant.
A suivre ..
12/05/2011
Anesthésie au poste de secours
Si vous devez faire des gestes chirurgicaux simples, il faudra avoir recours à une anesthésie. ATTENTION la règle numéro 1: Primum non nocere. C'est un métier. La sécurité est le premier objectif. Vous n'êtes pas formé pour cela, mais vous serez peut être placé devant l'obligation de mettre en oeuvre une anesthésie compte tenu du contexte. Le manuel qui suit est un grand classique.
Activité chirurgicale au poste de secours
Vous serez amené très certainement à intervenir auprès de la population pour la réalisation d'actes chirurgicaux simples. Le document qui vous est proposé est un grand classique, à lire et à relire et prendre ce qui peut être pris.
07/05/2011
Biomatériaux pour le contrôle des hémorragies
Surtout pour les hémorragies compressibles.
Une revue très détaillée sur les biomatériaux utilisés pour cet usage. (ici)
Hypothermie et traumatisé ne font pas bon ménage
Il est parfaitement démontré que l'hypothermie aggrave le pronostic vital des polytraumatisés. C'est un facteur indépendant de mortalité. Cette nouvelle publication le confirme. Elle précise par ailleurs que le risque d'hypothermie est accrue par un transport héliporté.
-------------------------------------------------
The incidence and significance of accidental hypothermia in major trauma—A prospective observational study
Ireland S et all.
Resuscitation 82 (2011) 300–306
Background
Serious sequelae have been associated with injured patients who are hypothermic (<35 °C) including coagulopathy, acidosis, decreased myocardial contractility and risk of mortality.
Aim
Establish the incidence of accidental hypothermia in major trauma patients and identify causative factors.
Method
Prospective identification and subsequent review of 732 medical records of major trauma patients presenting to an Adult Major Trauma Centre was undertaken between January and December 2008. Multivariate analysis was performed using logistic regression. Significant and clinically relevant variables from univariate analysis were entered into multivariate models to evaluate determinants for hypothermia and for death. Goodness of fit was determined with the use of the Hosmer–Lemeshow statistic.
Main results
Overall mortality was 9.15%. The incidence of hypothermia was 13.25%. The mortality of patients with hypothermia was 29.9% with a threefold independent risk of death: OR (CI 95%) 3.44 (1.48–7.99), P = 0.04. Independent determinants for hypothermia were pre-hospital intubation: OR (CI 95%) 5.18 (2.77–9.71), P < 0.001, Injury Severity Score (ISS): 1.04 (1.01–1.06), P = 0.01, Arrival Systolic Blood Pressure (ASBP) < 100 mm Hg: 3.04 (1.24–7.44), P = 0.02, and wintertime: 1.84 (1.06–3.21), P = 0.03.
Of the 87 hypothermic patients who had repeat temperatures recorded in the Emergency Department, 77 (88.51%) patients had a temperature greater than the recorded arrival temperature. There was no change in recorded temperature for four (4.60%) patients, whereas six (6.90%) patients were colder at Emergency Department discharge.
Conclusion
Seriously injured patients with accidental hypothermia have a higher mortality independent of measured risk factors. For patients with multiple injuries a coordinated effort by paramedics, nurses and doctors is required to focus efforts toward early resolution of hypothermia aiming to achieve a temperature >35 °C.
06/05/2011
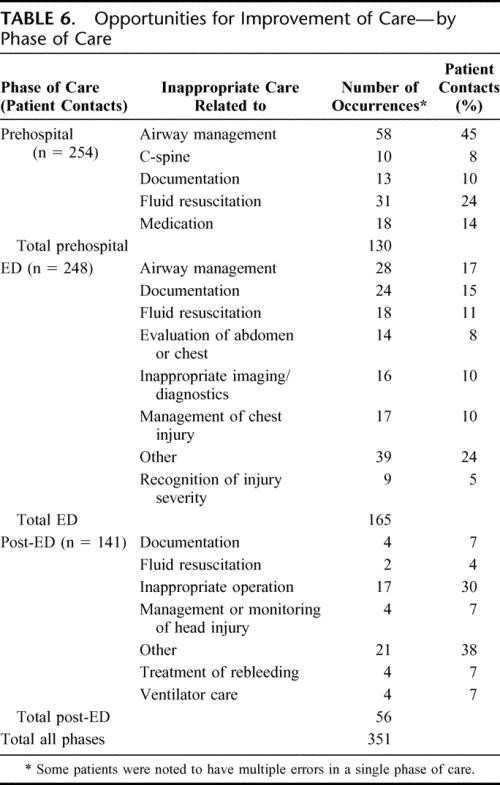
Mieux maîtriser les voies aériennes: Un axe majeur pour réduire la motalité préhospitalière du traumatisé
Analysis of Preventable Trauma Deaths and Opportunities for Trauma Care Improvement in Utah
Rachis: Immobilisation et plaies cervicales par balle
Unstable Cervical Spine Fracture After Penetrating Neck Injury: A Rare Entity in an Analysis of 1,069 Patients
Lustenberger T. et All.
JTrauma. 2011;70:870–872
-------------------------------------------------
En gros pas besoin de mettre en place une minerve en cas de plaie du cou sauf si le blessé est incosncient ou présente des signes neurologiques périphériques.
-------------------------------------------------
Background: The value of cervical spine immobilization after penetrating trauma to the neck is the subject of lively debate. The purpose of this study was to review the epidemiology of unstable cervical spine injuries (CSI) after penetrating neck trauma in a large cohort of patients.
Methods: This is a retrospective analysis of patients admitted with penetrating neck injuries to a Level I trauma center from January 1996 through December 2008. A penetrating neck injury was defined as a gunshot wound (GSW) or stab wound (SW) between the clavicles and the base of the skull. Univariate and multivariate analyses were performed to investigate associations between injury mechanisms, the presence of CSI instability, and mortality. Risk factors independently associated with the presence of a CSI were identified.
Results: A total of 1,069 patients met inclusion criteria, of which 463 patients (43.3%) and 606 patients (56.7%) were sustaining GSW and SW, respectively. Overall, 65 patients (6.1%) were diagnosed with a CSI with a significantly higher incidence after GSWs compared with SWs (12.1% vs. 1.5%; p < 0.001). In four patients (0.4%), the CSI was considered unstable, all of them following GSW. All patients with unstable CSI had obvious neurologic deficits or altered mental status at the time of admission. Risk factors independently associated with the presence of a CSI were GSW to the neck and a Glasgow Coma Scale score.
Conclusion: The overall incidence of unstable CSI after penetrating trauma to the neck is exceedingly low at 0.4%. Following GSW to the neck, an unstable CSI was noted in
-------------------------------------------------
Détail de la publication:
-------------------------------------------------
In four patients (0.4%), the CSI was considered unstable, all of them after GSW to the neck (0.9% for GSW vs. 0% for SW; p = 0.035). All patients with unstable CSI had obvious neurologic deficits or altered mental status at the time of initial presentation: two patients presented with tetraplegia and two patients had a GCS score of 3 on admission with subsequent brain death during their SICU stay. Stabilization of the spine was performed in both patients with tetraplegia but was without significant neurologic recovery after surgery.