01/05/2017
Intraosseux ? Ne pas aller trop profond
Intramedullary placement of intraosseous cannulas inserted in the preclinical treatment of polytrauma patients : A retrospective, computed tomography-assisted evaluation
Jansen Get Al. Anaesthesist. 2017 Mar;66(3):168-176
-------------------------------
Le recours à la voie intra-osseuse trouve a sa place lors de la prise en charge de traumatisé sévère. Il faut néanmoins s'assurer du bon positionnement intra-médullaire de l'aiguille. Ce travail appelle à de la prudence car il met en évidence la fréquence de positionnements non optimaux notamment un peu trop profond. Une vérification régulière s'impose dans le contexte de la traumatologie sévère.
-------------------------------
BACKGROUND:
Use of intraosseous access to the vascular system is rare in the pre-hospital setting (<1%). However, as patients for which the use of an intraosseous device is indicated are usually in a critical condition, awareness of possible application errors is vital. A survey was performed to evaluate intramedullary needle placement by means of computed axial tomography.
METHODS:
In the period of 01/01/2011 to 31/12/2015 all multislice-CT trauma scans performed in a trauma center were monitored for intraosseous devices in situ. The placement site, type of intraosseous device and needle deployed, thickness of bone and soft tissues, site for optimum needle placement, and both deviation from gold standard placement and visible complications were also recorded.
RESULTS:
In 11 out of 982 patients with suspected polytrauma that were studied during the observation period, 13 intraosseous cannulas were found (1.12%). In all cases, the EZ-IO® (Teleflex, P.O. Box 12600, Research Triangle Park, NC 27709, USA) intraosseous vascular access system was used. All applications were placed correctly in the medullary cavity, but none concurred with the current guidelines: The site of the puncture deviated laterally in seven cases, medially in two cases, cranially in four cases, and caudally in two cases.
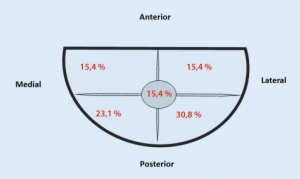
The most common error in all 13 cases was overshooting during needle introduction.
CONCLUSION:
Even though clinical criteria may suggest correct placement of an intraosseous device, the results of this survey provide evidence that deviations in positioning are common. Placement of the needle too deep can cause complications within the soft tissues or potentially impede intraosseous infusion.
| Tags : intraosseux
Les commentaires sont fermés.