15/06/2016
Coniotomie: Chirurgicale SVP !
Emergency Cricothyrotomy Performed by Surgical Airway–naive Medical Personnel
Heymans F. et Al. Anesthesiology 2016; 125:00-00
----------------------------------------
L'obstruction des voies aériennes est une cause rare mais évitable de décès au combat. savoir ouvrir un cou est donc un geste qui doit être maîtrisé par le médecin ou l'infirmier présent. Se pose cependant la question de la méthode: chirurgicale ou dispositif spécifique ? Ce travail apporte clairement une réponse. Des personnels de santé novice obtiennent de meilleurs résultats avec la technique chirurgicale. Même si la technique utilisée n'est pas celle promue par la procédure du sauvetage au combat (emploi d'un crochet de hook au lieu d'une pince de Monro-Kelly), ce travail conforte le choix qui est fait d'avoir recours à la technique chirurgicale.
----------------------------------------
Background: When conventional approaches to obtain effective ventilation and return of effective spontaneous breathing fail, surgical airway is the last rescue option. Most physicians have a limited lifetime experience with cricothyrotomy, and it is unclear what method should be taught for this lifesaving procedure. The aim of this study is to compare the performance of medical personnel, naive to surgical airway techniques, in establishing an emergency surgical airway in cadavers using three commonly used cricothyrotomy techniques.
Methods: Twenty medical students, without previous knowledge of surgical airway techniques, were randomly selected from their class. After training, they performed cricothyrotomy by three techniques (surgical, Merkel, and QuickTrach II) in a random order on 60 cadavers with comparable biometrics. The time to complete the procedure, rate of success, and number of complications were recorded. A success was defined as the correct placement of the cannula within the trachea in 3min.
"After intact skin palpation of relevant structures (step 1), a vertical midline skin incision (step 2) is emphasized because it can be extended up or down if not correctly placed and because fewer vessels are located at the midline. Although
rarely emphasized, we recommend finger palpation through the subcutaneous tissue (step 3) and even in the trachea as a guide, as a dissector, and as a dilator; finger palpation is oblivious to bleeding and a better guide to the ligament, being the “surgeon’s eye” during cricothyrotomy. A horizontal incision of the lower aspect of the cricotracheal ligament (step 4) allows for tension release and better opening. A hook permits to maintain the skin and the tracheal opening. Caudal traction (step 5) is recommended because the cricoid cartilage is more resistant and in order to prevent laryngeal injuries. We did not use a dilator, forceps, or a retractor during this experiment. Finally, a cuffed cannula is inserted (step 6)"
Results: The success rates were 95, 55, and 50% for surgical cricothyrotomy, QuickTrach, and Merkel, respectively (P = 0.025).
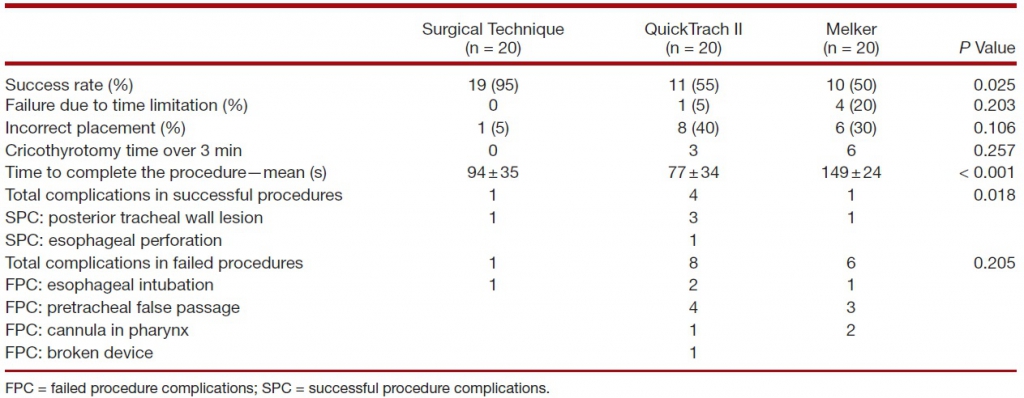
The majority of failures were due to cannula misplacement (15 of 20). In successful procedures, the mean procedure time was 94± 35 s in the surgical group, 77 ± 34 in the QuickTrach II group, and 149 ±24 in the Melker group (P < 0.001). Few significant complications were found in successful procedures. No cadaver biometric parameters were correlated with success of the procedure.
Conclusion: Surgical airway–naive medical personnel establish emergency cricothyrotomy more efficiently and safely with the surgical procedure than with the other two commonly used techniques
| Tags : airway
Les commentaires sont fermés.