02/12/2025
Les drones changent la donne
20/11/2025
Chaine de survie 21ème siècle: Réflexions US
Clic sur l'image pour accéder au document
Le facteur humain reste CENTRAL
"While technology continues to transform warfare, the human element remains central to military medicine. The operational ‘kill chain’ may be accelerated by drones and artificial intelligence. However, the medical ‘survival chain’ still demands human judgement, compassion, and moral courage"
19/01/2023
Le drone: Incontournable !
Drones reduce the treatment-free interval in search and rescue operations with telemedical support – A randomized control trial
Van Veelen MJ et Al. https://doi.org/10.1016/j.ajem.2023.01.020
------------------------------------
Un outil sans nul doute à maîtriser à la lumière des événements ukrainiens
------------------------------------
Introduction
Response to medical incidents in mountainous areas is delayed due to the remote and challenging terrain. Drones could assist in a quicker search for patients and can facilitate earlier treatment through delivery of medical equipment. We aim to assess the effects of drone deployment in search and rescue (SAR) operations in challenging terrain. We hypothesize that drones can reduce the search time and treatment-free interval of patients through initiation of telemedicine in a single mission.
Methods
In this randomized control trial with a cross-over design two methods of searching for and initiating treatment of a patient were compared. The primary outcome was a comparison of the times for locating a patient through visual contact and starting treatment on-site between the drone assisted intervention arm and the conventional ground rescue control arm. A linear mixed model (LMM) was used to evaluate the effect of using a drone on search and start of treatment times.
Results
Twenty-four SAR missions, performed by six SAR teams each with four team members, were analyzed. The mean time to locate the patient was 14.6 min (95% CI 11.3–17.9) in the drone assisted intervention arm and 20.6 min (95% CI 17.3–23.9) in the control arm. The mean time to start treatment was 15.7 min (95% CI 12.4–19.0) in the drone assisted arm and 22.4 min (95% CI 19.1–25.7) in the control arm ( p < 0.01 for both comparisons).

Conclusion
Drone deployment in SAR operations leads to a reduction in search time and treatment-free interval of patients in challenging terrain, which could improve outcomes in patients suffering from traumatic injuries, the most commonly occurring incident requiring mountain rescue deployment.
| Tags : drone
16/04/2019
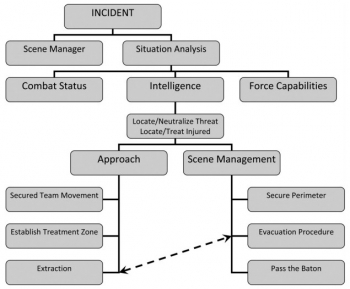
TCCC: Un écosystème spécifique
Un regard sur l'émergence des nouvelles modalités de prise en charge des blessés de guerre avec pour point d'orgue l'innovation conduite et la construction d'un écosystème complet autour de la prise en charge du blessé de guerre. Une démarche à comprendre et à bien méditer.
Clic sur l'image pour accéder au document
15/09/2018
Aggressions collectives par arme de guerre
08/09/2018
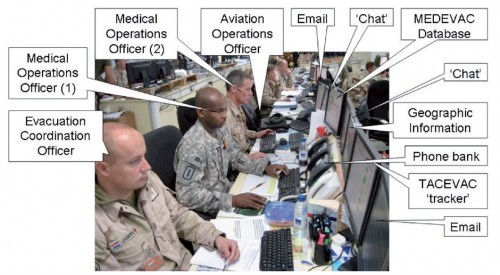
Le TCCC dans la vraie vie
Survey of Casualty Evacuation Missions Conducted by the 160th Special Operations Aviation Regiment During the Afghanistan Conflict.
BACKGROUND:
Historically, documentation of prehospital combat casualty care has been relatively nonexistent. Without documentation, performance improvement of prehospital care and evacuation through data collection, consolidation, and scientific analyses cannot be adequately accomplished. During recent conflicts, prehospital documentation has received increased attention for point-of-injury care as well as for care provided en route on medical evacuation platforms. However, documentation on casualty evacuation (CASEVAC) platforms is still lacking. Thus, a CASEVAC dataset was developed and maintained by the 160th Special Operations Aviation Regiment (SOAR), a nonmedical, rotary-wing aviation unit, to evaluate and review CASEVAC missions conducted by their organization.
METHODS:
A retrospective review and descriptive analysis were performed on data from all documented CASEVAC missions conducted in Afghanistan by the 160th SOAR from January 2008 to May 2015. Documentation of care was originally performed in a narrative after-action review (AAR) format. Unclassified, nonpersonally identifiable data were extracted and transferred from these AARs into a database for detailed analysis. Data points included demographics, flight time, provider number and type, injury and outcome details, and medical interventions provided by ground forces and CASEVAC personnel.
RESULTS:
There were 227 patients transported during 129 CASEVAC missions conducted by the 160th SOAR. Three patients had unavailable data, four had unknown injuries or illnesses, and eight were military working dogs. Remaining were 207 trauma casualties (96%) and five medical patients (2%). The mean and median times of flight from the injury scene to hospital arrival were less than 20 minutes. Of trauma casualties, most were male US and coalition forces (n = 178; 86%). From this population, injuries to the extremities (n = 139; 67%) were seen most commonly. The primary mechanisms of injury were gunshot wound (n = 89; 43%) and blast injury (n = 82; 40%). The survival rate was 85% (n = 176) for those who incurred trauma. Of those who did not survive, most died before reaching surgical care (26 of 31; 84%).
CONCLUSION:
Performance improvement efforts directed toward prehospital combat casualty care can ameliorate survival on the battlefield. Because documentation of care is essential for conducting performance improvement, medical and nonmedical units must dedicate time and efforts accordingly. Capturing and analyzing data from combat missions can help refine tactics, techniques, and procedures and more accurately define wartime personnel, training, and equipment requirements. This study is an example of how performance improvement can be initiated by a nonmedical unit conducting CASEVAC missions.
06/06/2015
Prise en charge d'un blessé: Ce n'est pas le SAMU, ni la catastrophe
Tactical medicine: a joint forces field algorithm.
Waldman M et Al. Mil Med. 2014 Oct;179(10):1056-61
31/05/2013
Mieux on est formé, plus on fait
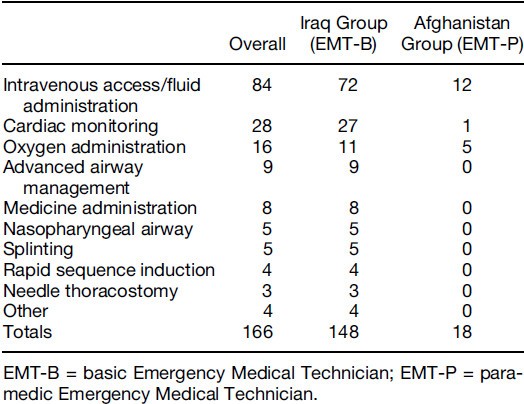
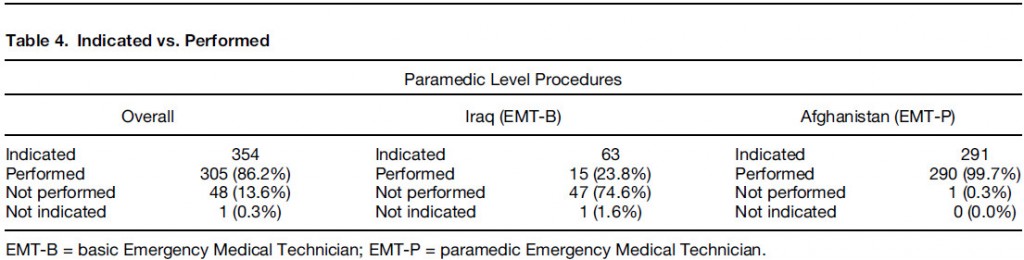
Army flight medic performance of paramedic level procedures: Indicated vs performed
Bier SA et all. - J Emerg Med. 2013 May;44(5):962-9.
Of 984 interventions found to be indicated on the 406 charts that met inclusion criteria, 36% were rated as EMT-P level. Seventeen percent were indicated but not performed. EMT-Bs failed to perform indicated procedures 35% of the time vs. 3% in the EMT-P group (p < 0.001). For paramedic-level procedures, EMTBs failed to make 76% of appropriate interventions, compared to <1% in the EMT-P group (p < 0.001). Conclusions: There seems to be a substantial number of procedures beyond the scope of standard Army flight medic training being required for Army AMT missions. It seems that when advance interventions are indicated, those trained to the EMT-P level perform them significantly more often than those trained to Army standard. Conclusions: Based on the findings of this study, the authors suggest the Army consider adopting the standards required for civilian AMT
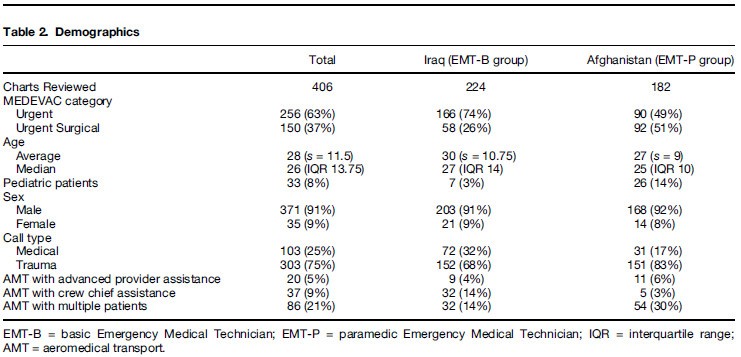
Commentaire:Notez la part de pédiatrie
Commentaire: EMT-B = Auxilaire sanitaire. EMT P = Technicien de niveau plutôt infirmiers formés exclusivement à la gestion de soins critiques. Pas d'équivalence avec la vision française (entre infirmier anesthésiste/réa ?)
Ceci milite pour la présence dans les vecteurs d'EVASAN notamment aériens de personnels paramédicaux spécifiques habitués à la mise en oeuvre de standards de soins critiques
| Tags : evasan
29/09/2012
L'essence du triage
Ce témoignage exprime parfaitement tous les enjeux du sauvetage au combat en montrant qu'il s'agit d'un concept de prise en charge intégrant toutes les dimensions dela traumatologie moderne (préparation, savoir faire personnel, travail en équipe: son équipe et les autres, délégation, leadership, gestion du stress).
Etre fort dans sa tête, dans son savoir pour pouvoir former ses personnels et les guider au moment de l'action en ayant pris le recul suffisant.
| Tags : triage, leadership, pédagogie, mascal
03/06/2012
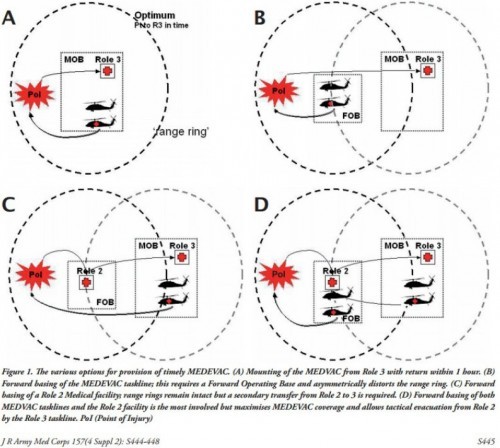
Evasan: la vision anglo-saxone
Chaîne santé: Un positionnement idéal ?
Forward Medical Evacuation
Bricknell MCM et all. J R Army Med Corps 157(4 Suppl 2): S444-448
The "right patient, right platform, right escort, right time, right place"
Derrière tout cela une organisation