05/05/2012
Ready heat ou triple couche ?
The effect of active warming in prehospital trauma care during road and air ambulance transportation - a clinical randomized trial.
Lundgren P. et all Scand J Trauma Resusc Emerg Med. 2011 Oct 21;19:59.
La prévention de l'hypothermie fait appel à des moyens de réchauffement cutanés passifs ( couverture renforcée type Rothco ou la couverture triple couche type blizzard blanket ) ou actifs (couverture ready-heat). Mais comment choisir ?
Le travail présenté ici démontre qu'en présence d'une hypothermie modérée supérieures à 35°C il n'est pas utile d'avoir recours à un moyen actif en terme de limitation de l'hypothermie dès lors que le frisson est conservé. Le seul gain porte sur un confort thermique accru.
BACKGROUND:
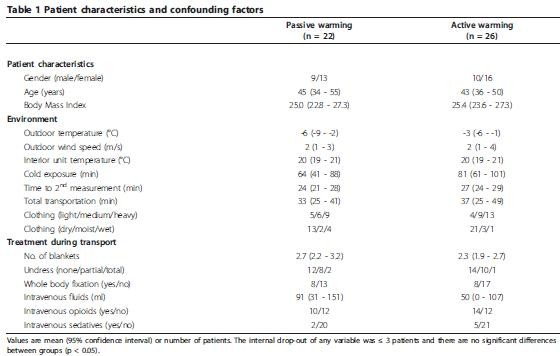
Prevention and treatment of hypothermia by active warming in prehospital trauma care is recommended but scientific evidence of its effectiveness in a clinical setting is scarce. The objective of this study was to evaluate the effect of additional active warming during road or air ambulance transportation of trauma patients.
METHODS:
Patients were assigned to either passive warming with blankets or passive warming with blankets with the addition of an active warming intervention using a large chemical heat pad applied to the upper torso. Ear canal temperature, subjective sensation of cold discomfort and vital signs were monitored.
RESULTS:
Mean core temperatures increased from 35.1°C (95% CI; 34.7-35.5°C) to 36.0°C (95% CI; 35.7-36.3°C) (p < 0.05) in patients assigned to passive warming only (n = 22) and from 35.6°C (95% CI; 35.2-36.0°C) to 36.4°C (95% CI; 36.1-36.7°C) (p < 0.05) in patients assigned to additional active warming (n = 26) with no significant differences between the groups. Cold discomfort decreased in 2/3 of patients assigned to passive warming only and in all patients assigned to additional active warming, the difference in cold discomfort change being statistically significant (p < 0.05). Patients assigned to additional active warming also presented a statistically significant decrease in heart rate and respiratory frequency (p < 0.05).
CONCLUSIONS:
In mildly hypothermic trauma patients, with preserved shivering capacity, adequate passive warming is an effective treatment to establish a slow rewarming rate and to reduce cold discomfort during prehospital transportation. However, the addition of active warming using a chemical heat pad applied to the torso will significantly improve thermal comfort even further and might also reduce the cold induced stress response.
| Tags : hypothermie
Les commentaires sont fermés.