02/12/2025
Les drones changent la donne
09/10/2024
Combat à haute intensité: Tout repenser !
Casualty care implications of large-scale combat operations
Mason H. Remondelli MH et Al. J Trauma Acute Care Surg. 2023 Aug; 95(2 ): S180–S184.
----------------------------------------------------------------------------------
Cet article met en exergue la nécessité de repenser en profondeur l'organisation de la chaîne santé , la place prépondérante de la transfusion sanguine et l'intérêt de petites équipes chirurgicales mobiles intervenant "enterrées" au plus près des combats
----------------------------------------------------------------------------------

02/04/2024
Les gestes US du Role 1 chez les américains
An Analysis of 13 Years of Prehospital Combat Casualty Care: Implications for Maintaining a Ready Medical Force
Schauer SG et Al. Prehosp Emerg Care. 2022 May-Jun;26(3):370-379.
----------------------------------
Des choses simples dans un contexte où les medevac étaient très rapides, ce qui n'est plus le cas. Poser des garrots est toujours nécessaires MAIS ne suffit plus. Les gestes sophistiqués de réanimation doivent absolument être maîtrisées. Cela passe par une autre vision, que celle actuelle, de la médicalisation de l'avant.
----------------------------------
Background:
Most potentially preventable deaths occur in the prehospital setting before reaching a military treatment facility with surgical capabilities. Thus, optimizing the care we deliver in the prehospital combat setting represents a ripe target for reducing mortality. We sought to analyze prehospital data within the Department of Defense Trauma Registry (DODTR).
Materials and methods:
We requested all encounters with any prehospital activity (e.g., interventions, transportation, vital signs) documented within the DODTR from January 2007 to March 2020 along with all hospital-based data that was available. We excluded from our search casualties that had no prehospital activity documented.
Results:
There were 28,950 encounters that met inclusion criteria. Of these, 25,897 (89.5%) were adults and 3053 were children (10.5%). There was a steady decline in the number of casualties encountered with the most notable decline occurring in 2014. U.S. military casualties comprised the largest proportion (n = 10,182) of subjects followed by host nation civilians (n = 9637). The median age was 24 years (interquartile range/IQR 21-29).
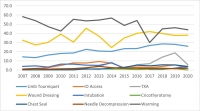
Most were battle injuries (78.6%) and part of Operation ENDURING FREEDOM (61.8%) and Operation IRAQI FREEDOM (24.4%). Most sustained injuries from explosives (52.1%) followed by firearms (28.1%), with serious injury to the extremities (24.9%) occurring most frequently. The median injury severity score was 9 (IQR 4-16) with most surviving to discharge (95.0%). A minority had a documented medic or combat lifesaver (27.9%) in their chain of care, nor did they pass through an aid station (3.0%). Air evacuation predominated (77.9%).
Conclusions:
Within our dataset, the deployed U.S. military medical system provided prehospital medical care to at least 28,950 combat casualties consisting mostly of U.S. military personnel and host nation civilian care. There was a rapid decline in combat casualty volumes since 2014, however, on a per-encounter basis there was no apparent drop in procedural volume.
15/03/2024
Plus d'infirmiers spécialisés dans le trauma
Une évidence. Et dans le système français le modèle de cet infirmier est un IADE
ACNPs in the U.S. Army-Medical Force Multipliers for Large-Scale Combat Operations
16/02/2022
Triage en cas d'attaque terroriste: Des limites
Triage in Complex, Coordinated Terrorist Attacks
Pepper M et Al. Prehosp Disaster Med. 2019 Aug;34(4):442-448.
Introduction:
Terror attacks have increased in frequency, and tactics utilized have evolved. This creates significant challenges for first responders providing life-saving medical care in their immediate aftermath. The use of coordinated and multi-site attack modalities exacerbates these challenges. The use of triage is not well-validated in mass-casualty settings, and in the setting of intentional mass violence, new and innovative approaches are needed.
Methods:
Literature sourced from gray and peer-reviewed sources was used to perform a comparative analysis on the application of triage during the 2011 Oslo/Utoya Island (Norway), 2015 Paris (France), and 2015 San Bernardino (California USA) terrorist attacks. A thematic narrative identifies strengths and weaknesses of current triage systems in the setting of complex, coordinated terrorist attacks (CCTAs).
Discussion:
Triage systems were either not utilized, not available, or adapted and improvised to the tactical setting. The complexity of working with large numbers of patients, sensory deprived environments, high physiological stress, and dynamic threat profiles created significant barriers to the implementation of triage systems designed around flow charts, physiological variables, and the use of tags. Issues were identified around patient movement and "tactical triage."
Conclusion:
Current triage tools are inadequate for use in insecure environments, such as the response to CCTAs. Further research and validation are required for novel approaches that simplify tactical triage and support its effective application. Simple solutions exist in tactical triage, patient movement, and tag use, and should be considered as part of an overall triage system.
| Tags : triage
20/01/2018
Queensland Clinical Practice Manual

Clic sur l'image pour accéder aux protocoles
15/08/2015
Quel médecin en role 1 ?
Perceptions of Frontline Providers on the Appropriate Qualifi cations for Battalion Level Care in United States Army Ground Maneuver Forces
Malish RG et Al. Military Medicine, 176, 12:1369, 2011
--------------------------------
Il est habituel pour nous qu'un médecin déployé en role 1 soit un médecin généraliste. Ce n'est pas le cas dans d'autres armées notamment l'armée américaine où d'une part des spécialistes hospitaliers et d'autre part des officiers de santé ("physician assistant, souvent ancien combat medic) peuvent être déployés en role 1.
--------------------------------
Objectives: